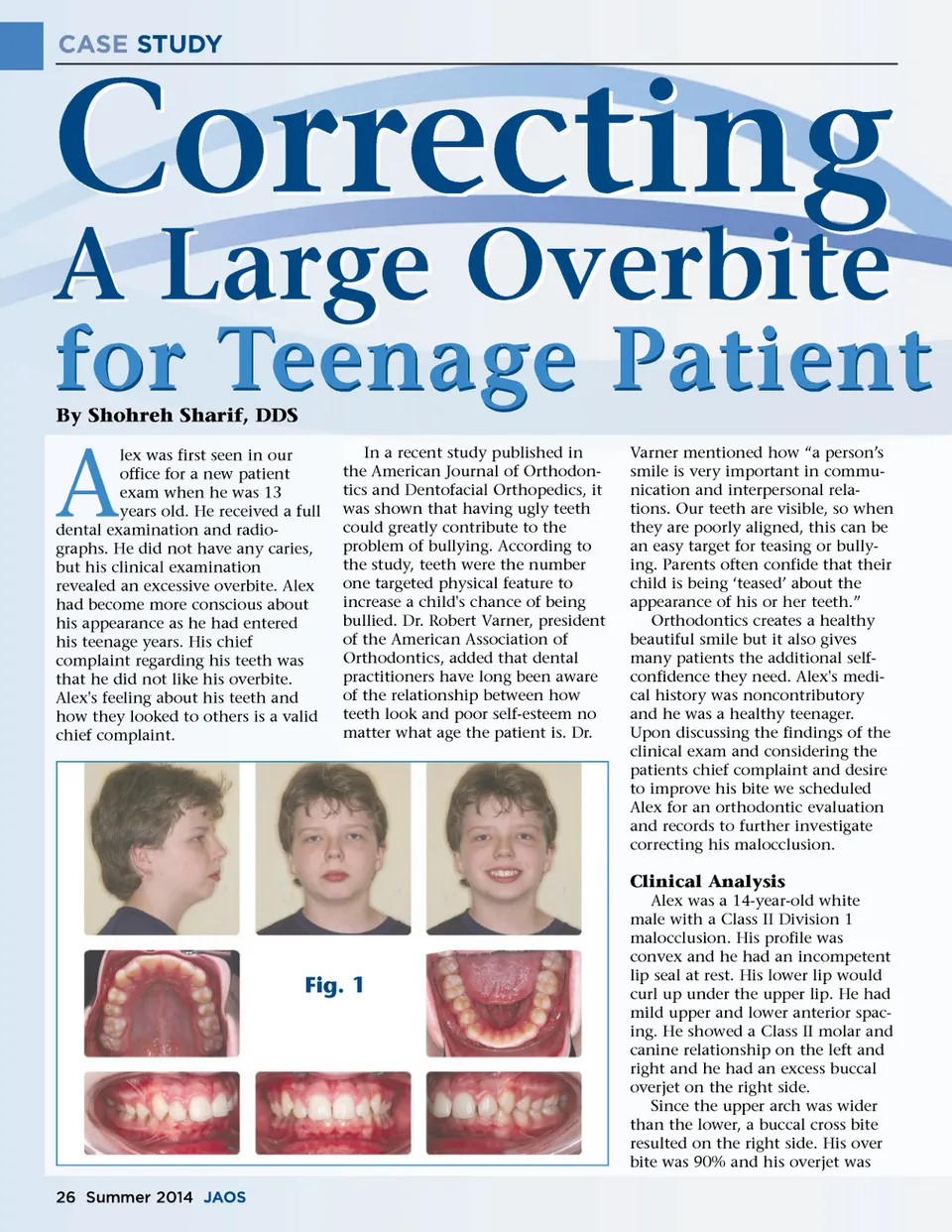
CASE STUDY Correcting A Large Overbite By Shohreh Sharif, DDS for Teenage Patient A lex was first seen in our office for a new patient exam when he was 13 years old. He received a full dental examination and radio-graphs. He did not have any caries, but his clinical examination revealed an excessive overbite. Alex had become more conscious about his appearance as he had entered his teenage years. His chief complaint regarding his teeth was that he did not like his overbite. Alex's feeling about his teeth and how they looked to others is a valid chief complaint. In a recent study published in the American Journal of Orthodon-tics and Dentofacial Orthopedics, it was shown that having ugly teeth could greatly contribute to the problem of bullying. According to the study, teeth were the number one targeted physical feature to increase a child's chance of being bullied. Dr. Robert Varner, president of the American Association of Orthodontics, added that dental practitioners have long been aware of the relationship between how teeth look and poor self-esteem no matter what age the patient is. Dr. Varner mentioned how “a person’s smile is very important in commu-nication and interpersonal rela-tions. Our teeth are visible, so when they are poorly aligned, this can be an easy target for teasing or bully-ing. Parents often confide that their child is being ‘teased’ about the appearance of his or her teeth.” Orthodontics creates a healthy beautiful smile but it also gives many patients the additional self-confidence they need. Alex's medi-cal history was noncontributory and he was a healthy teenager. Upon discussing the findings of the clinical exam and considering the patients chief complaint and desire to improve his bite we scheduled Alex for an orthodontic evaluation and records to further investigate correcting his malocclusion. Clinical Analysis Alex was a 14-year-old white male with a Class II Division 1 malocclusion. His profile was convex and he had an incompetent lip seal at rest. His lower lip would curl up under the upper lip. He had mild upper and lower anterior spac-ing. He showed a Class II molar and canine relationship on the left and right and he had an excess buccal overjet on the right side. Since the upper arch was wider than the lower, a buccal cross bite resulted on the right side. His over bite was 90% and his overjet was Fig. 1 26 Summer 2014 JAOS
Journal of the American Orthodontic Society Summer 2014 / Buyer's Guide: Page 26