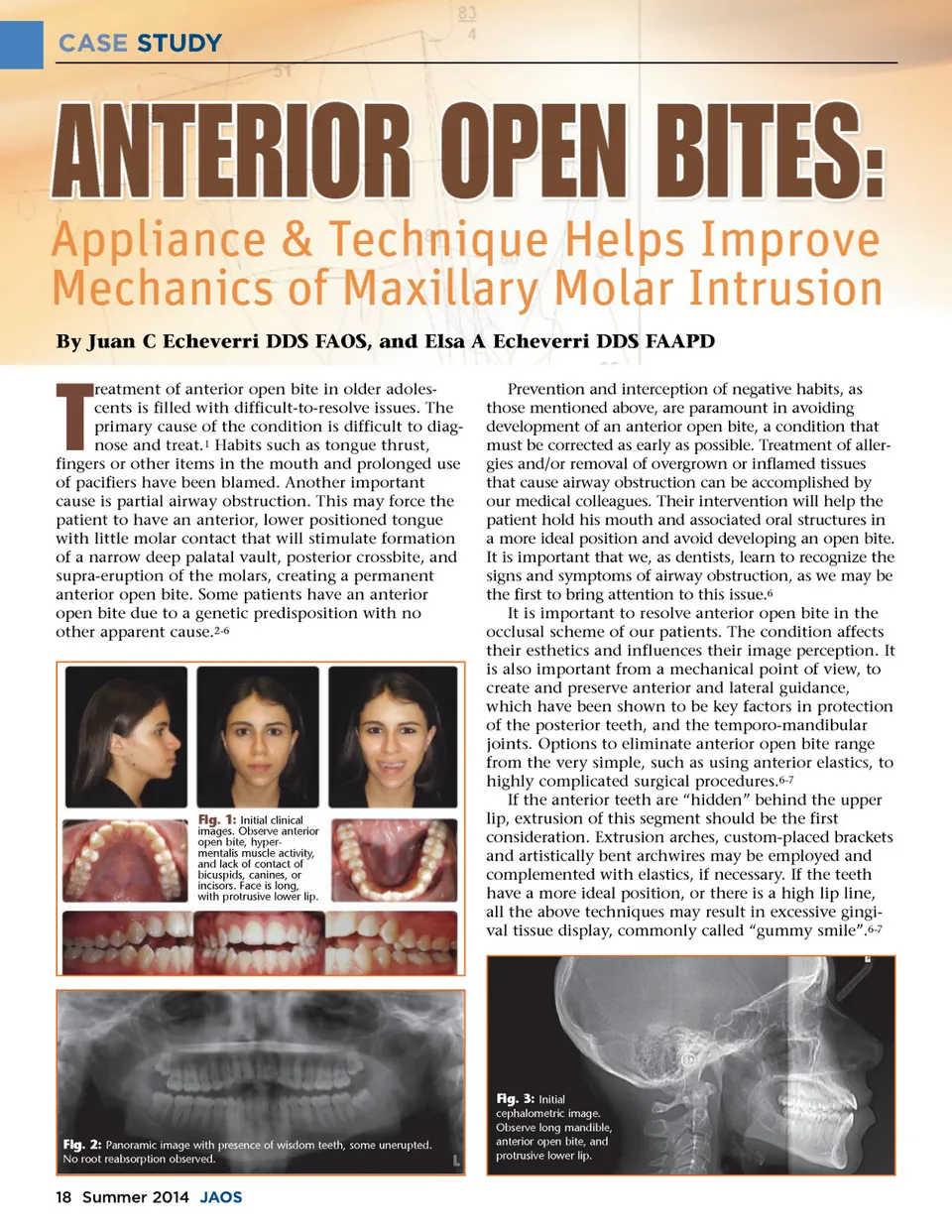
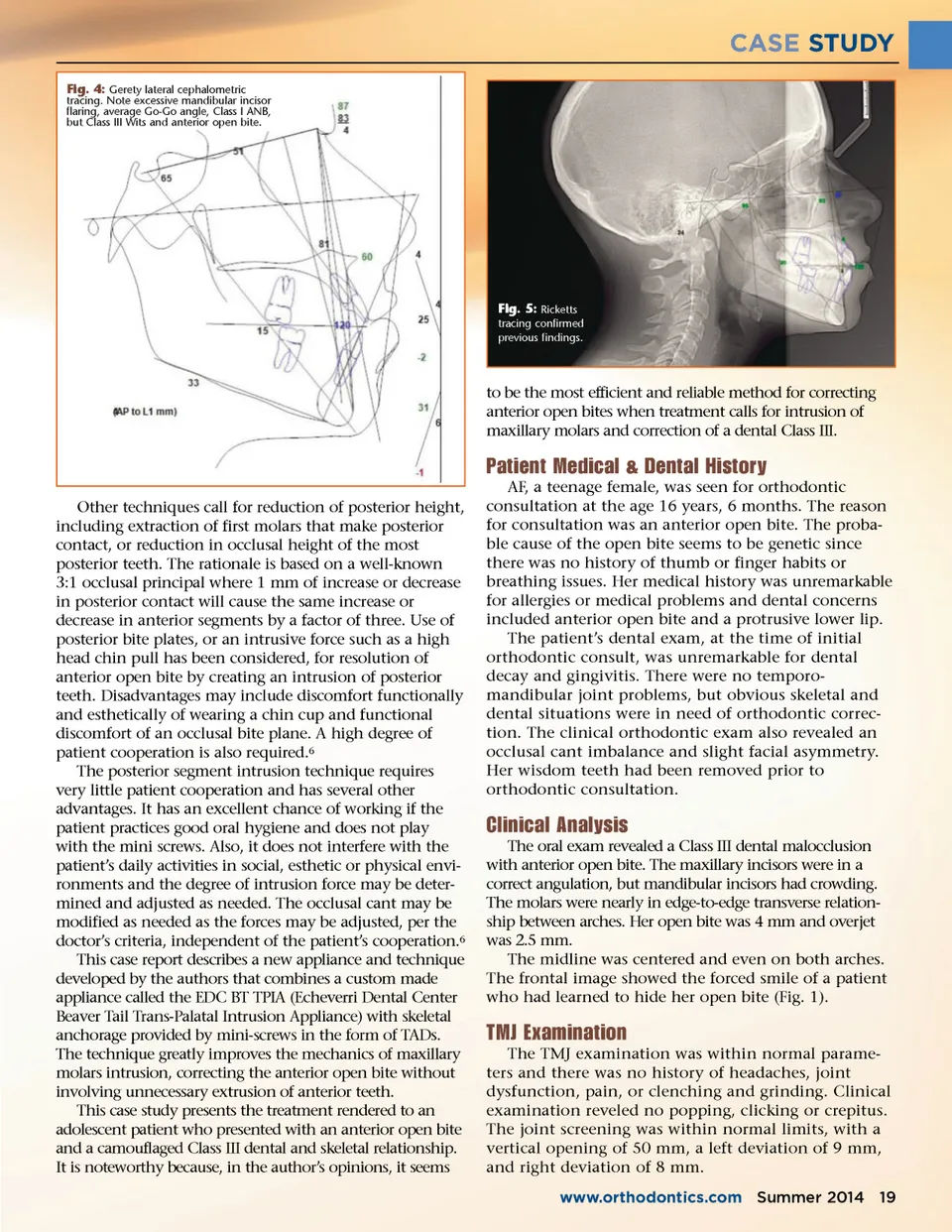
CASE STUDY By Juan C Echeverri DDS FAOS, and Elsa A Echeverri DDS FAAPD T reatment of anterior open bite in older adoles-cents is filled with difficult-to-resolve issues. The primary cause of the condition is difficult to diag-nose and treat. 1 Habits such as tongue thrust, fingers or other items in the mouth and prolonged use of pacifiers have been blamed. Another important cause is partial airway obstruction. This may force the patient to have an anterior, lower positioned tongue with little molar contact that will stimulate formation of a narrow deep palatal vault, posterior crossbite, and supra-eruption of the molars, creating a permanent anterior open bite. Some patients have an anterior open bite due to a genetic predisposition with no other apparent cause. 2-6 Fig. 1: Initial clinical images. Observe anterior open bite, hyper-mentalis muscle activity, and lack of contact of bicuspids, canines, or incisors. Face is long, with protrusive lower lip. Prevention and interception of negative habits, as those mentioned above, are paramount in avoiding development of an anterior open bite, a condition that must be corrected as early as possible. Treatment of aller-gies and/or removal of overgrown or inflamed tissues that cause airway obstruction can be accomplished by our medical colleagues. Their intervention will help the patient hold his mouth and associated oral structures in a more ideal position and avoid developing an open bite. It is important that we, as dentists, learn to recognize the signs and symptoms of airway obstruction, as we may be the first to bring attention to this issue. 6 It is important to resolve anterior open bite in the occlusal scheme of our patients. The condition affects their esthetics and influences their image perception. It is also important from a mechanical point of view, to create and preserve anterior and lateral guidance, which have been shown to be key factors in protection of the posterior teeth, and the temporo-mandibular joints. Options to eliminate anterior open bite range from the very simple, such as using anterior elastics, to highly complicated surgical procedures. 6-7 If the anterior teeth are “hidden” behind the upper lip, extrusion of this segment should be the first consideration. Extrusion arches, custom-placed brackets and artistically bent archwires may be employed and complemented with elastics, if necessary. If the teeth have a more ideal position, or there is a high lip line, all the above techniques may result in excessive gingi-val tissue display, commonly called “gummy smile”. 6-7 Fig. 2: Panoramic image with presence of wisdom teeth, some unerupted. No root reabsorption observed. Fig. 3: Initial cephalometric image. Observe long mandible, anterior open bite, and protrusive lower lip. 18 Summer 2014 JAOS
Journal of the American Orthodontic Society Summer 2014 / Buyer's Guide: Page 18