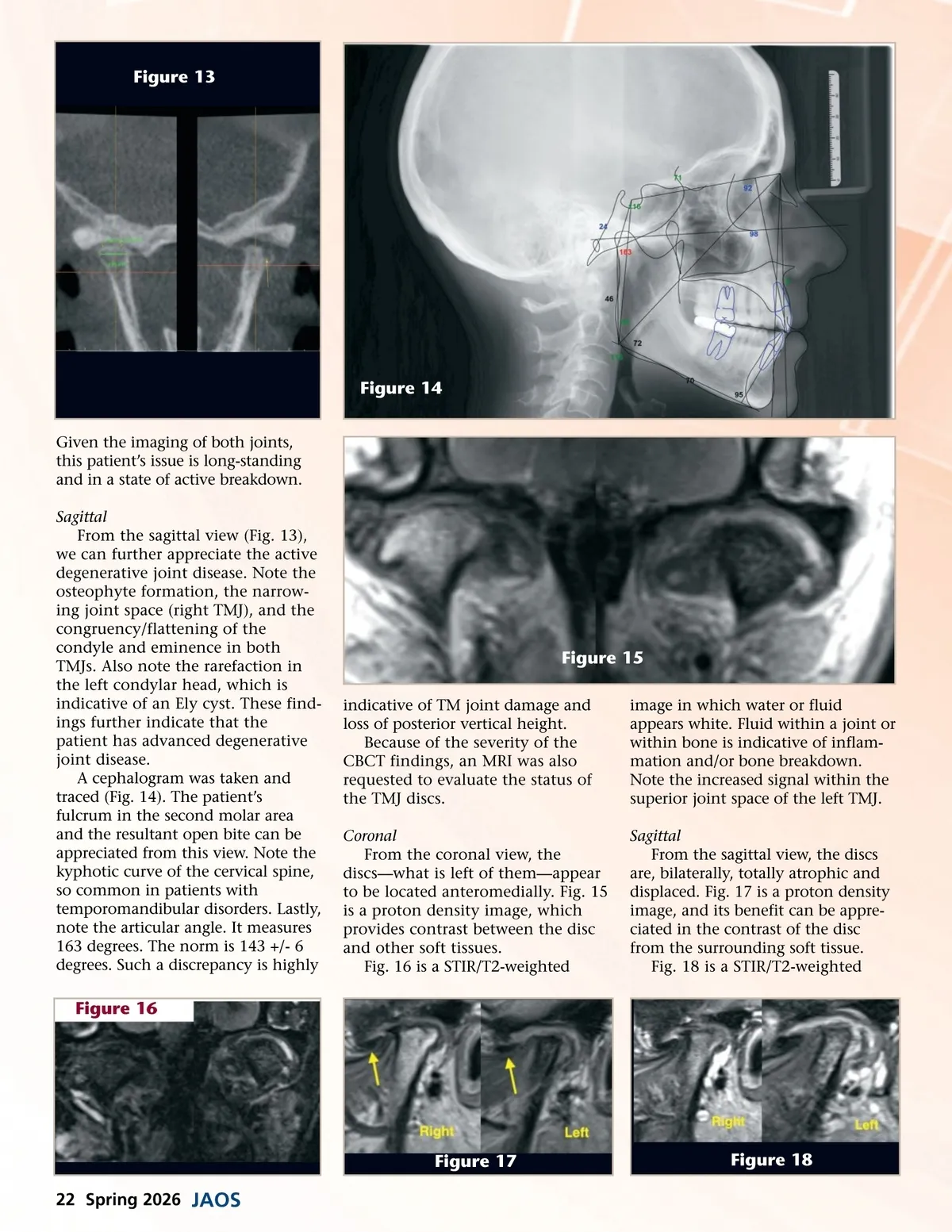
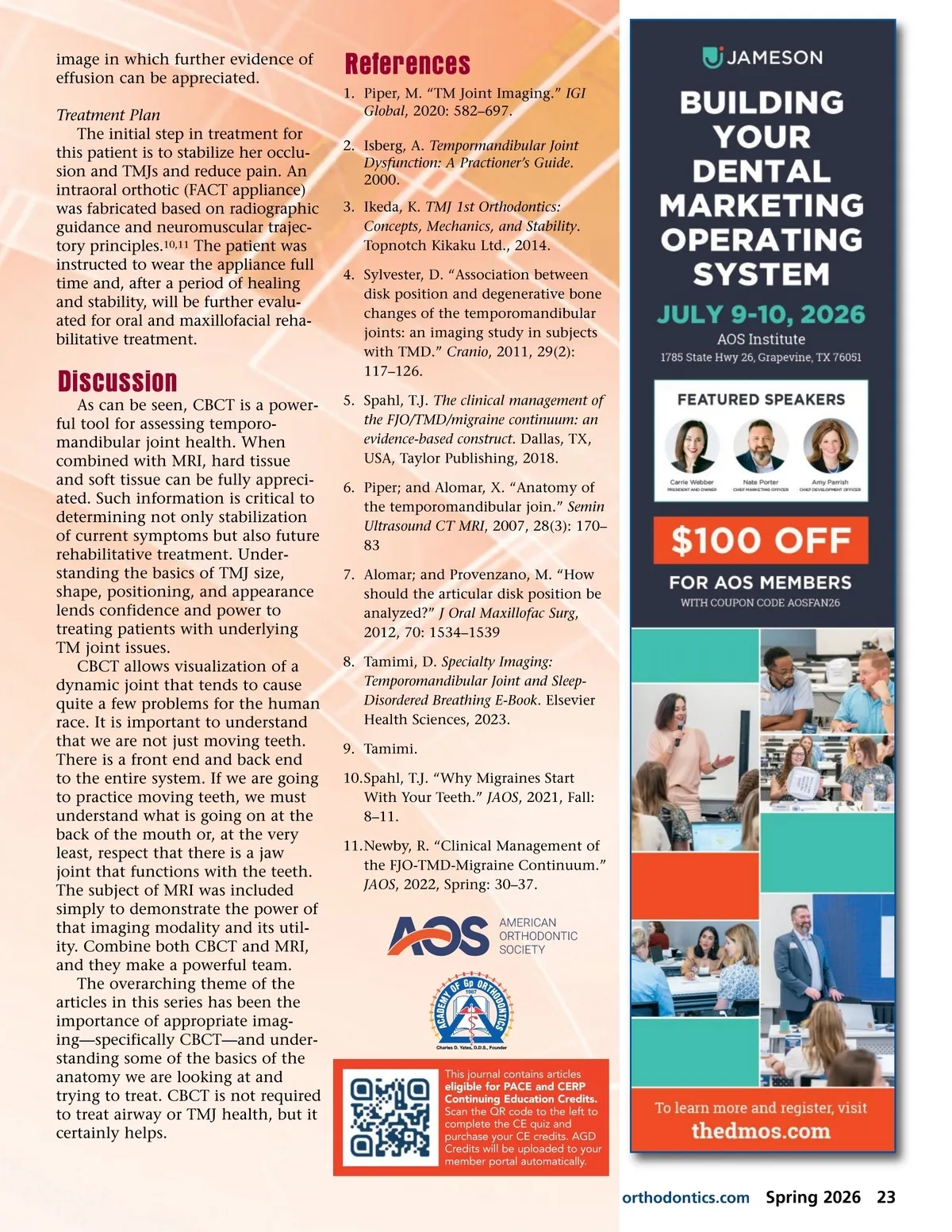
Figure 13 Figure 14 Given the imaging of both joints, this patient’s issue is long-standing and in a state of active breakdown. Sagittal From the sagittal view (Fig. 13), we can further appreciate the active degenerative joint disease. Note the osteophyte formation, the narrow-ing joint space (right TMJ), and the congruency/flattening of the condyle and eminence in both TMJs. Also note the rarefaction in the left condylar head, which is indicative of an Ely cyst. These find-ings further indicate that the patient has advanced degenerative joint disease. A cephalogram was taken and traced (Fig. 14). The patient’s fulcrum in the second molar area and the resultant open bite can be appreciated from this view. Note the kyphotic curve of the cervical spine, so common in patients with temporomandibular disorders. Lastly, note the articular angle. It measures 163 degrees. The norm is 143 +/-6 degrees. Such a discrepancy is highly Figure 15 indicative of TM joint damage and loss of posterior vertical height. Because of the severity of the CBCT findings, an MRI was also requested to evaluate the status of the TMJ discs. Coronal From the coronal view, the discs—what is left of them—appear to be located anteromedially. Fig. 15 is a proton density image, which provides contrast between the disc and other soft tissues. Fig. 16 is a STIR/T2-weighted image in which water or fluid appears white. Fluid within a joint or within bone is indicative of inflam-mation and/or bone breakdown. Note the increased signal within the superior joint space of the left TMJ. Sagittal From the sagittal view, the discs are, bilaterally, totally atrophic and displaced. Fig. 17 is a proton density image, and its benefit can be appre-ciated in the contrast of the disc from the surrounding soft tissue. Fig. 18 is a STIR/T2-weighted Figure 16 Figure 17 22 Spring 2026 JAOS Figure 18
Journal of the American Orthodontic Society Spring 2026: Page 22