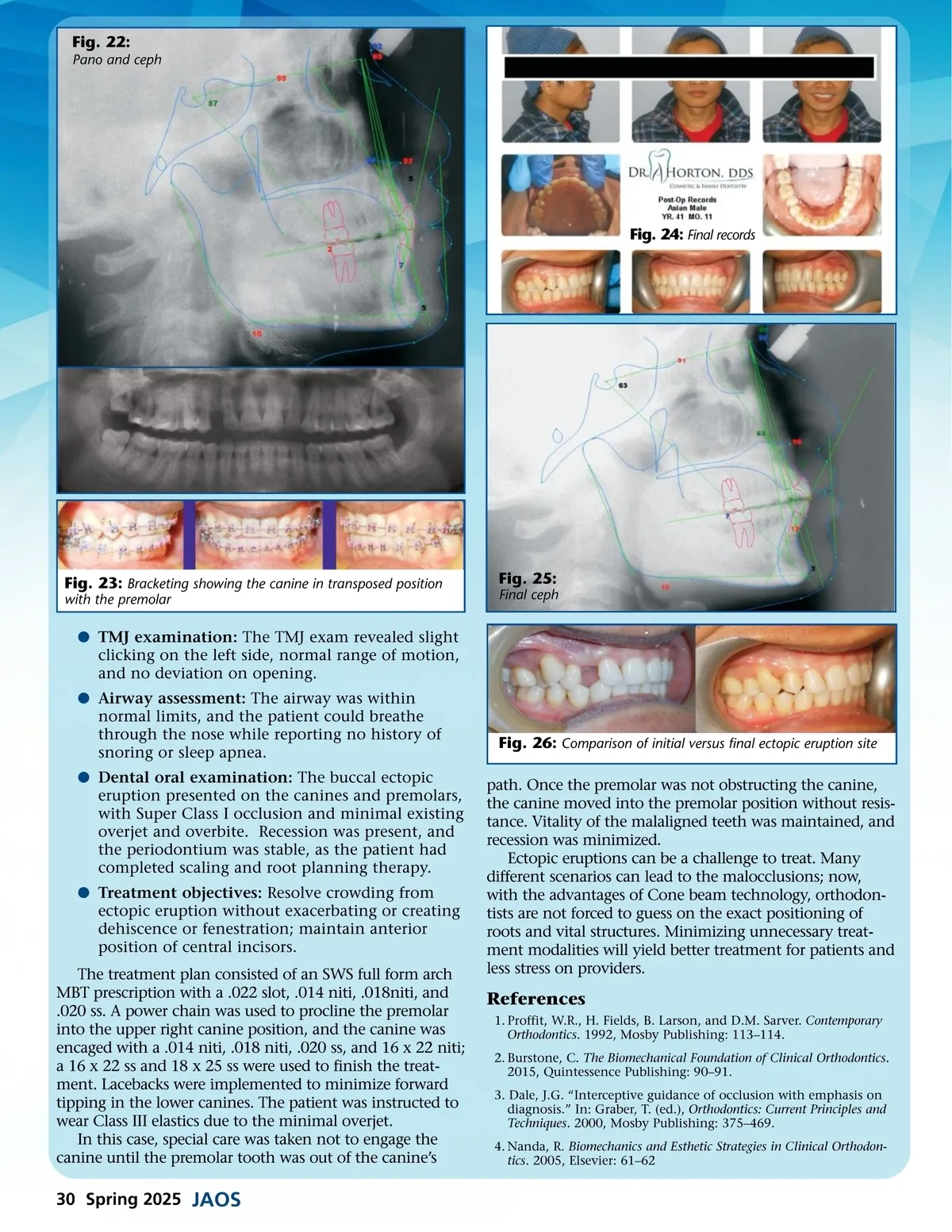
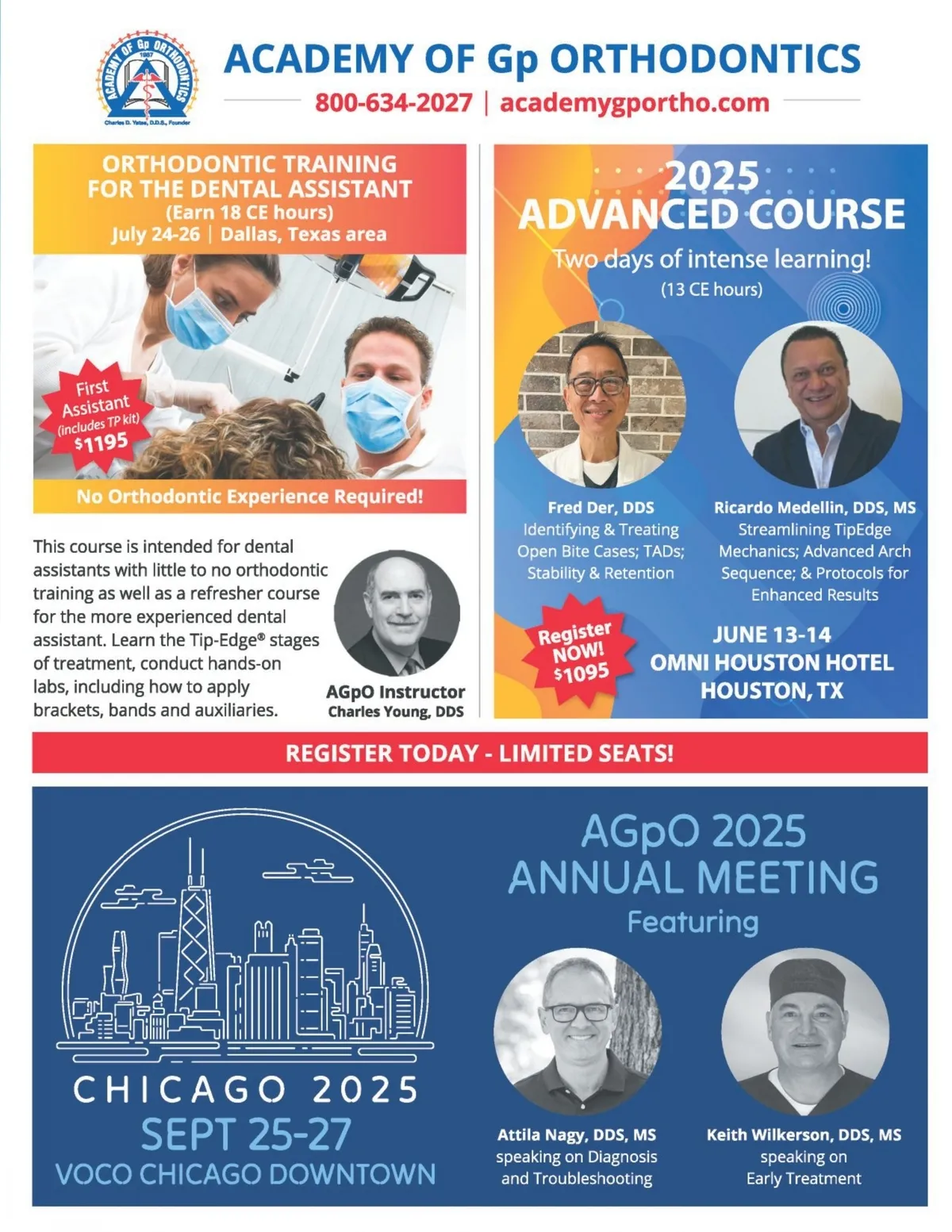
Fig. 22: Pano and ceph Fig. 24: Final records Fig. 23: Bracketing showing the canine in transposed position with the premolar Fig. 25: Final ceph b TMJ examination: The TMJ exam revealed slight clicking on the left side, normal range of motion, and no deviation on opening. b Airway assessment: The airway was within normal limits, and the patient could breathe through the nose while reporting no history of snoring or sleep apnea. b Dental oral examination: The buccal ectopic eruption presented on the canines and premolars, with Super Class I occlusion and minimal existing overjet and overbite. Recession was present, and the periodontium was stable, as the patient had completed scaling and root planning therapy. b Treatment objectives: Resolve crowding from ectopic eruption without exacerbating or creating dehiscence or fenestration; maintain anterior position of central incisors. The treatment plan consisted of an SWS full form arch MBT prescription with a .022 slot, .014 niti, .018niti, and .020 ss. A power chain was used to procline the premolar into the upper right canine position, and the canine was encaged with a .014 niti, .018 niti, .020 ss, and 16 x 22 niti; a 16 x 22 ss and 18 x 25 ss were used to finish the treat-ment. Lacebacks were implemented to minimize forward tipping in the lower canines. The patient was instructed to wear Class III elastics due to the minimal overjet. In this case, special care was taken not to engage the canine until the premolar tooth was out of the canine’s Fig. 26: Comparison of initial versus final ectopic eruption site path. Once the premolar was not obstructing the canine, the canine moved into the premolar position without resis-tance. Vitality of the malaligned teeth was maintained, and recession was minimized. Ectopic eruptions can be a challenge to treat. Many different scenarios can lead to the malocclusions; now, with the advantages of Cone beam technology, orthodon-tists are not forced to guess on the exact positioning of roots and vital structures. Minimizing unnecessary treat-ment modalities will yield better treatment for patients and less stress on providers. References 1. Proffit, W.R., H. Fields, B. Larson, and D.M. Sarver. Contemporary Orthodontics . 1992, Mosby Publishing: 113–114. 2. Burstone, C. The Biomechanical Foundation of Clinical Orthodontics . 2015, Quintessence Publishing: 90–91. 3. Dale, J.G. “Interceptive guidance of occlusion with emphasis on diagnosis.” In: Graber, T. (ed.), Orthodontics: Current Principles and Techniques . 2000, Mosby Publishing: 375–469. 4. Nanda, R. Biomechanics and Esthetic Strategies in Clinical Orthodon-tics . 2005, Elsevier: 61–62 30 Spring 2025 JAOS
Journal of the American Orthodontic Society Spring 2025: Page 30