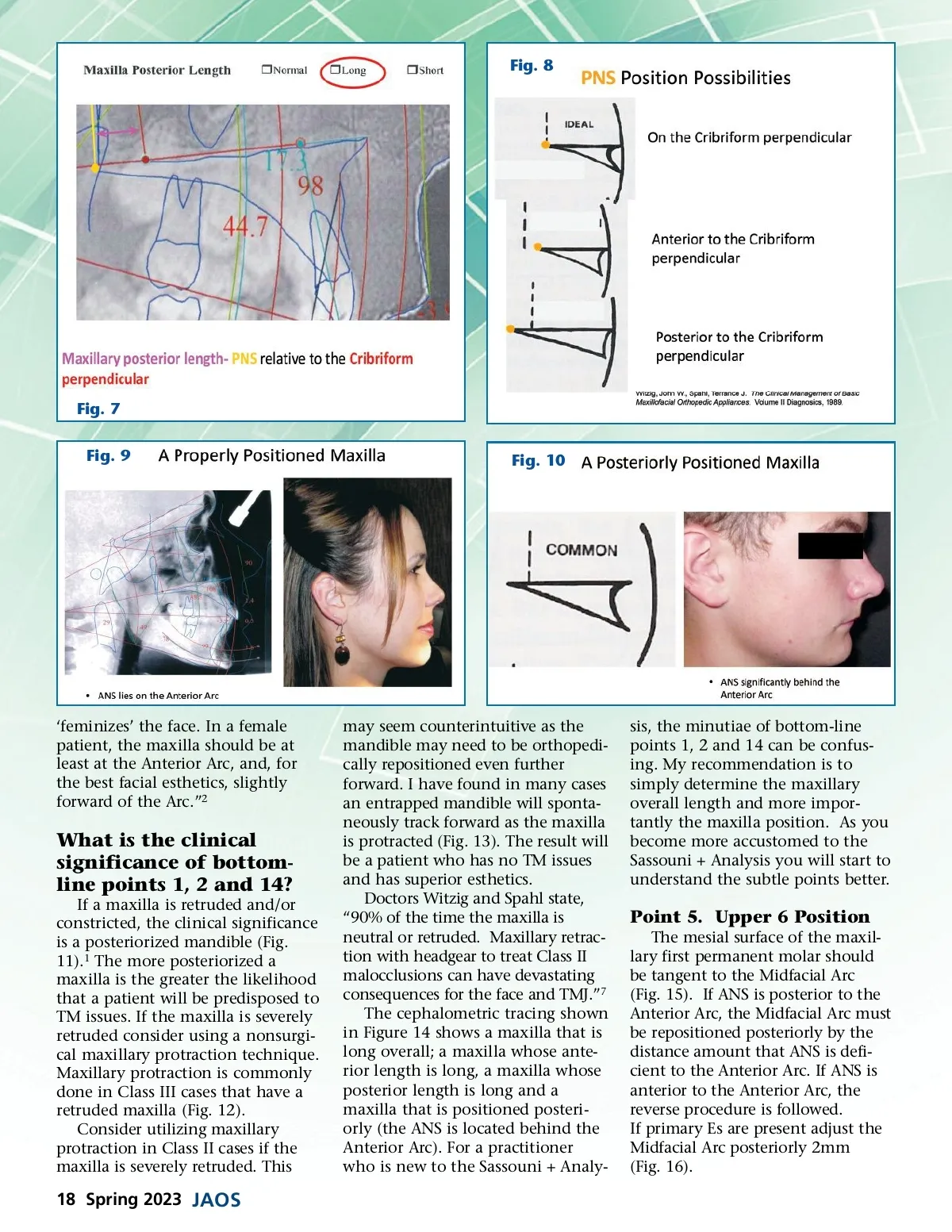
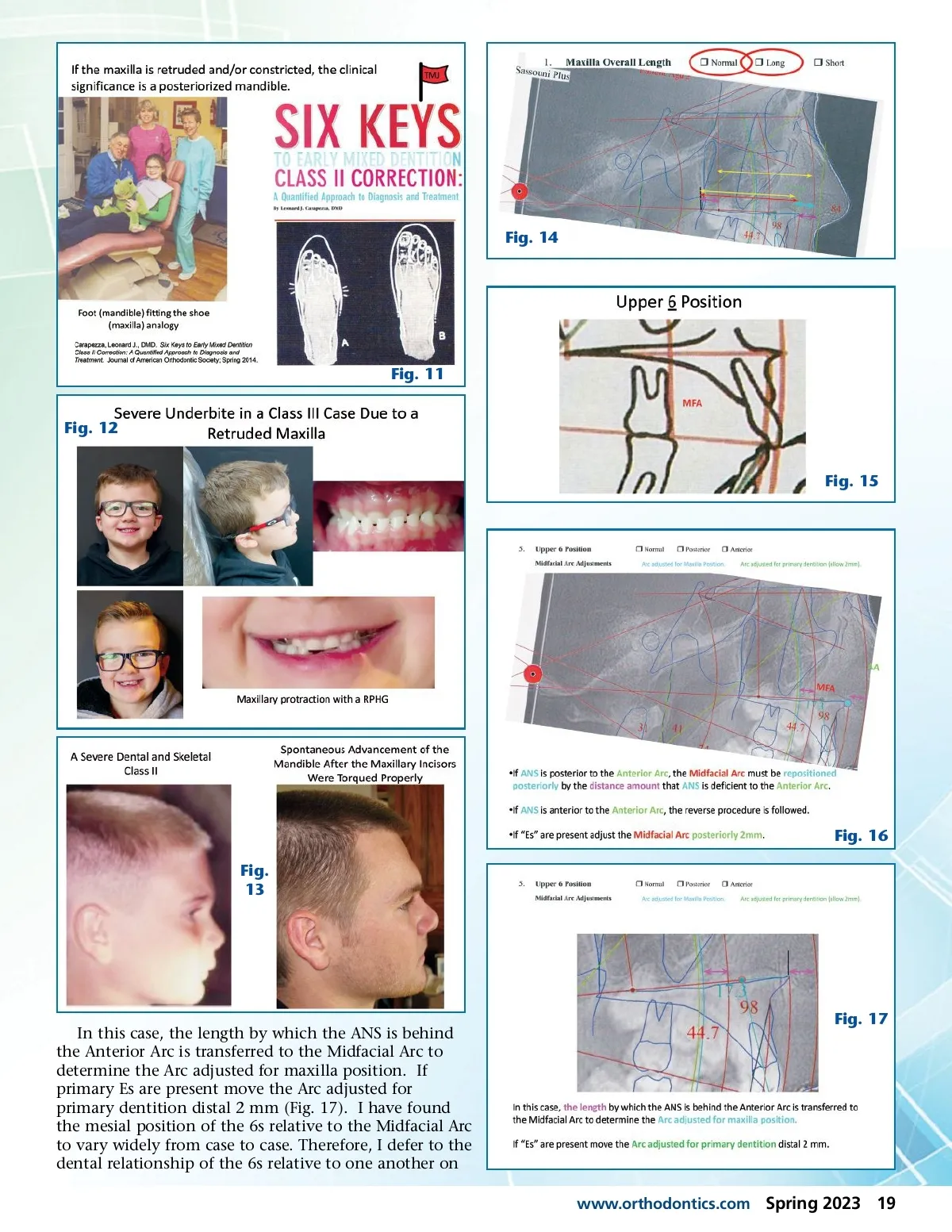
Fig. 8 Fig. 7 Fig. 9 Fig. 10 ‘feminizes’ the face. In a female patient, the maxilla should be at least at the Anterior Arc, and, for the best facial esthetics, slightly forward of the Arc.” 2 What is the clinical significance of bottom-line points 1, 2 and 14? If a maxilla is retruded and/or constricted, the clinical significance is a posteriorized mandible (Fig. 11). 1 The more posteriorized a maxilla is the greater the likelihood that a patient will be predisposed to TM issues. If the maxilla is severely retruded consider using a nonsurgi-cal maxillary protraction technique. Maxillary protraction is commonly done in Class III cases that have a retruded maxilla (Fig. 12). Consider utilizing maxillary protraction in Class II cases if the maxilla is severely retruded. This may seem counterintuitive as the mandible may need to be orthopedi-cally repositioned even further forward. I have found in many cases an entrapped mandible will sponta-neously track forward as the maxilla is protracted (Fig. 13). The result will be a patient who has no TM issues and has superior esthetics. Doctors Witzig and Spahl state, “90% of the time the maxilla is neutral or retruded. Maxillary retrac-tion with headgear to treat Class II malocclusions can have devastating consequences for the face and TMJ.” 7 The cephalometric tracing shown in Figure 14 shows a maxilla that is long overall; a maxilla whose ante-rior length is long, a maxilla whose posterior length is long and a maxilla that is positioned posteri-orly (the ANS is located behind the Anterior Arc). For a practitioner who is new to the Sassouni + Analy-sis, the minutiae of bottom-line points 1, 2 and 14 can be confus-ing. My recommendation is to simply determine the maxillary overall length and more impor-tantly the maxilla position. As you become more accustomed to the Sassouni + Analysis you will start to understand the subtle points better. Point 5. Upper 6 Position The mesial surface of the maxil-lary first permanent molar should be tangent to the Midfacial Arc (Fig. 15). If ANS is posterior to the Anterior Arc, the Midfacial Arc must be repositioned posteriorly by the distance amount that ANS is defi-cient to the Anterior Arc. If ANS is anterior to the Anterior Arc, the reverse procedure is followed. If primary Es are present adjust the Midfacial Arc posteriorly 2mm (Fig. 16). 18 Spring 2023 JAOS
Journal of the American Orthodontic Society Spring 2023: Page 18