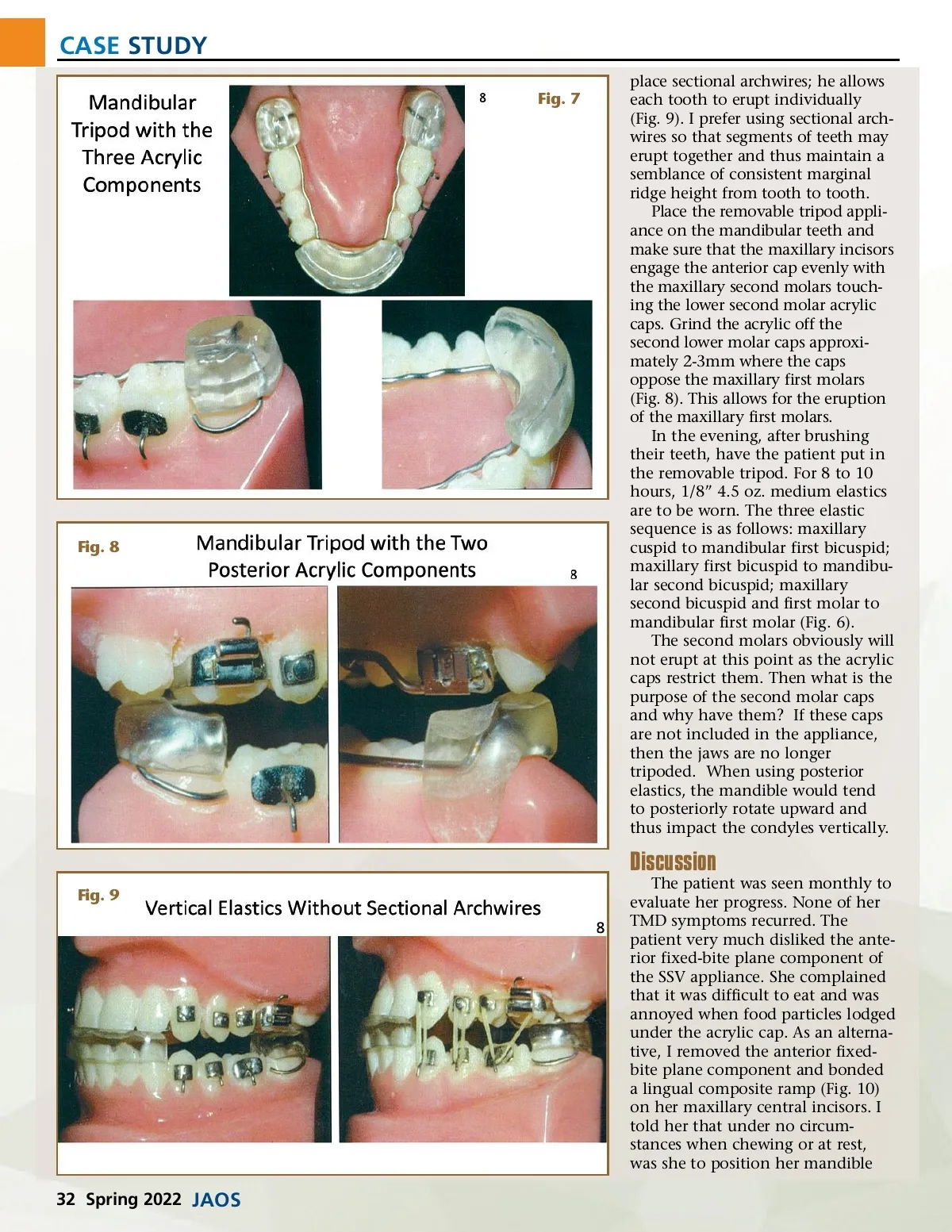
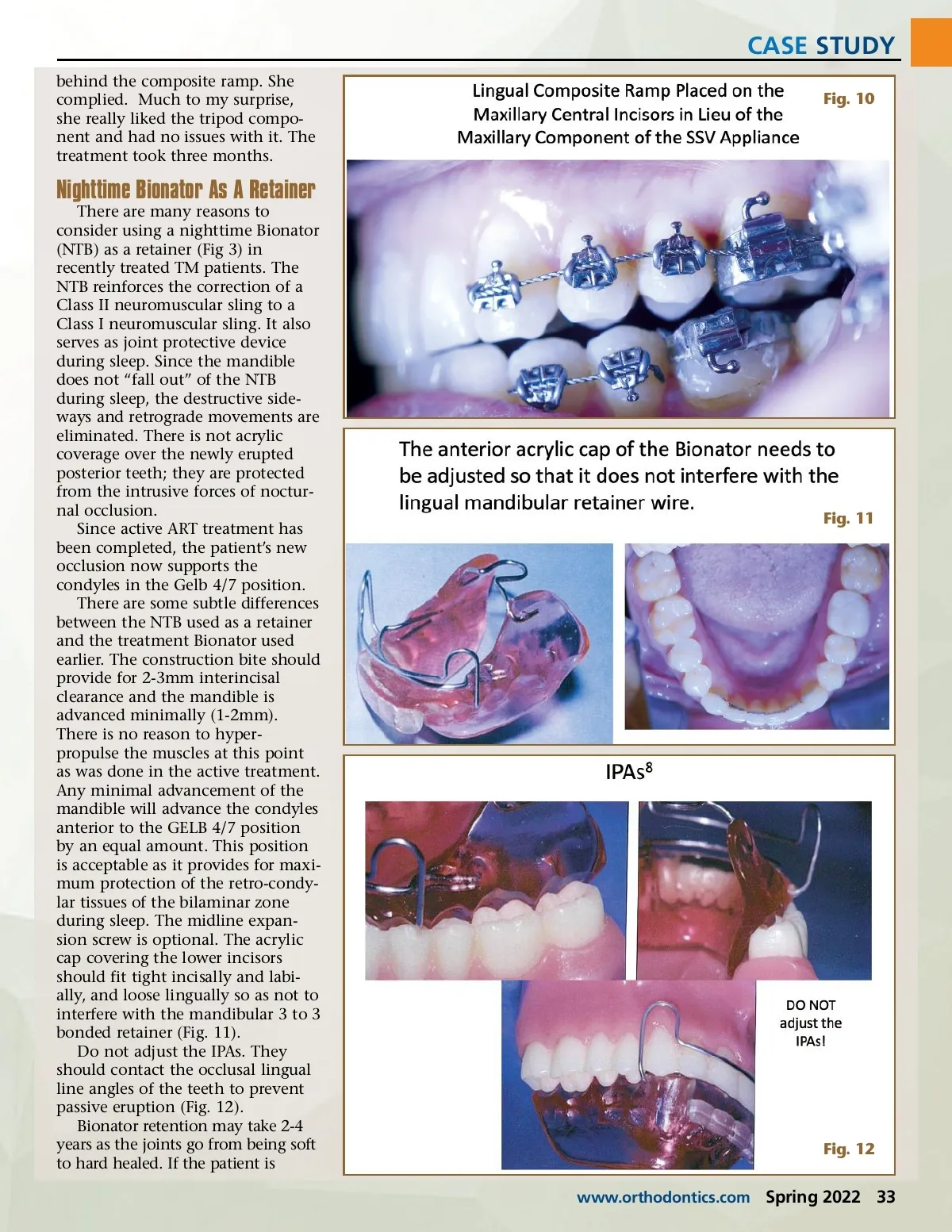
CASE STUDY behind the composite ramp. She complied. Much to my surprise, she really liked the tripod compo-nent and had no issues with it. The treatment took three months. Fig. 10 Nighttime Bionator As A Retainer There are many reasons to consider using a nighttime Bionator (NTB) as a retainer (Fig 3) in recently treated TM patients. The NTB reinforces the correction of a Class II neuromuscular sling to a Class I neuromuscular sling. It also serves as joint protective device during sleep. Since the mandible does not “fall out” of the NTB during sleep, the destructive side-ways and retrograde movements are eliminated. There is not acrylic coverage over the newly erupted posterior teeth; they are protected from the intrusive forces of noctur-nal occlusion. Since active ART treatment has been completed, the patient’s new occlusion now supports the condyles in the Gelb 4/7 position. There are some subtle differences between the NTB used as a retainer and the treatment Bionator used earlier. The construction bite should provide for 2-3mm interincisal clearance and the mandible is advanced minimally (1-2mm). There is no reason to hyper-propulse the muscles at this point as was done in the active treatment. Any minimal advancement of the mandible will advance the condyles anterior to the GELB 4/7 position by an equal amount. This position is acceptable as it provides for maxi-mum protection of the retro-condy-lar tissues of the bilaminar zone during sleep. The midline expan-sion screw is optional. The acrylic cap covering the lower incisors should fit tight incisally and labi-ally, and loose lingually so as not to interfere with the mandibular 3 to 3 bonded retainer (Fig. 11). Do not adjust the IPAs. They should contact the occlusal lingual line angles of the teeth to prevent passive eruption (Fig. 12). Bionator retention may take 2-4 years as the joints go from being soft to hard healed. If the patient is www.orthodontics.com Fig. 11 Fig. 12 Spring 2022 33
Journal of the American Orthodontic Society Spring 2022: Page 33