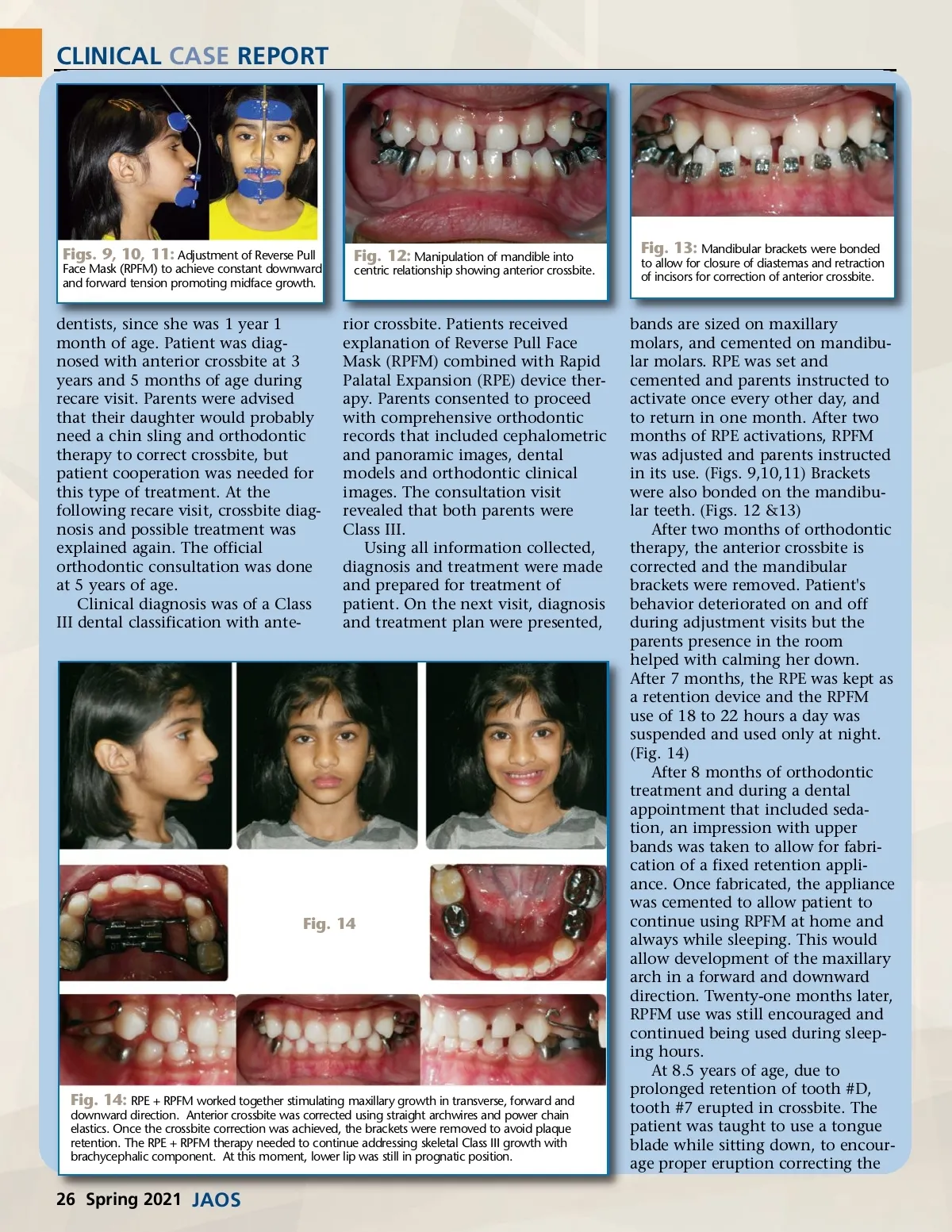
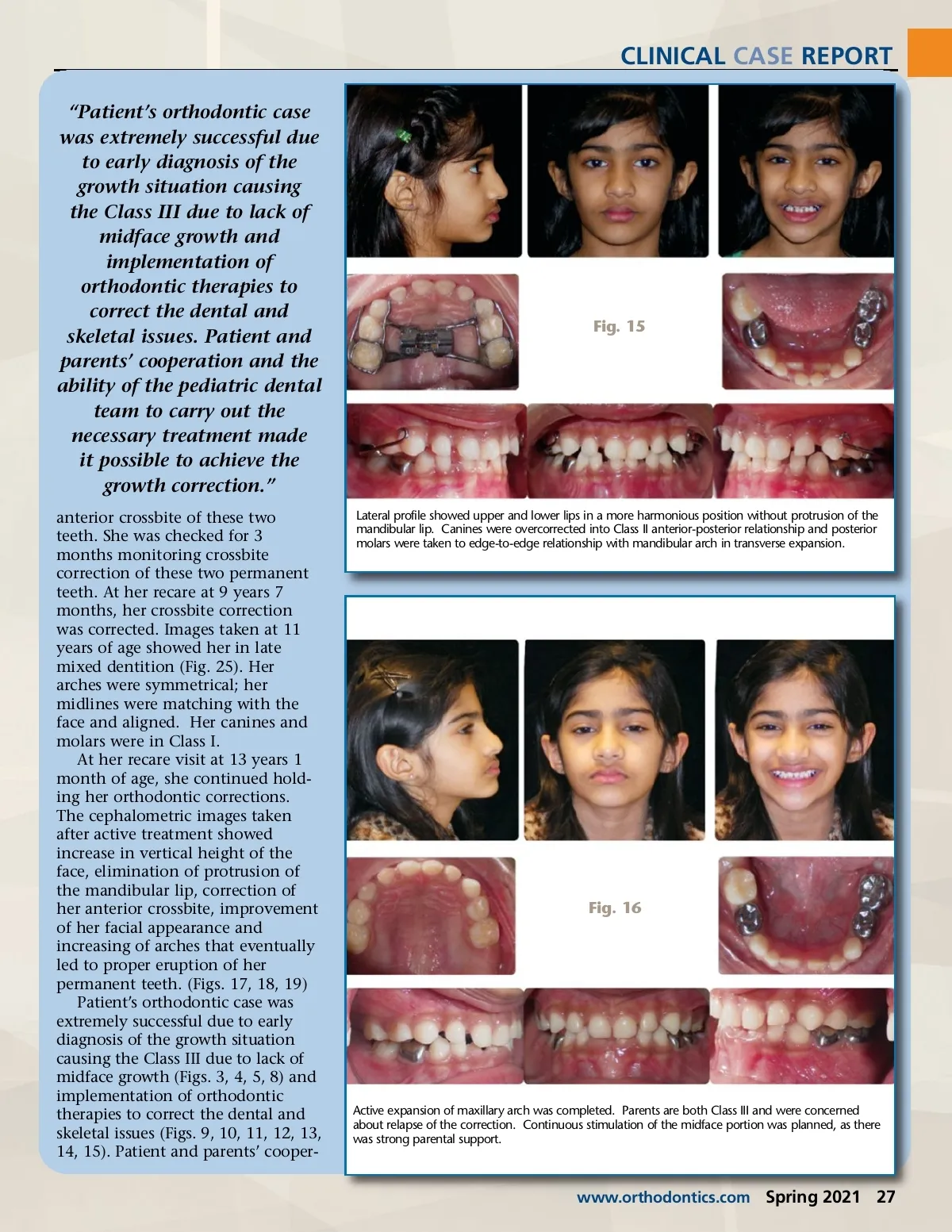
CLINICAL CASE REPORT Figs. 9, 10, 11: Adjustment of Reverse Pull Face Mask (RPFM) to achieve constant downward and forward tension promoting midface growth. dentists, since she was 1 year 1 month of age. Patient was diag-nosed with anterior crossbite at 3 years and 5 months of age during recare visit. Parents were advised that their daughter would probably need a chin sling and orthodontic therapy to correct crossbite, but patient cooperation was needed for this type of treatment. At the following recare visit, crossbite diag-nosis and possible treatment was explained again. The official orthodontic consultation was done at 5 years of age. Clinical diagnosis was of a Class III dental classification with ante-Fig. 12: Manipulation of mandible into centric relationship showing anterior crossbite. Fig. 13: Mandibular brackets were bonded to allow for closure of diastemas and retraction of incisors for correction of anterior crossbite. rior crossbite. Patients received explanation of Reverse Pull Face Mask (RPFM) combined with Rapid Palatal Expansion (RPE) device ther-apy. Parents consented to proceed with comprehensive orthodontic records that included cephalometric and panoramic images, dental models and orthodontic clinical images. The consultation visit revealed that both parents were Class III. Using all information collected, diagnosis and treatment were made and prepared for treatment of patient. On the next visit, diagnosis and treatment plan were presented, Fig. 14 Fig. 14: RPE + RPFM worked together stimulating maxillary growth in transverse, forward and downward direction. Anterior crossbite was corrected using straight archwires and power chain elastics. Once the crossbite correction was achieved, the brackets were removed to avoid plaque retention. The RPE + RPFM therapy needed to continue addressing skeletal Class III growth with brachycephalic component. At this moment, lower lip was still in prognatic position. bands are sized on maxillary molars, and cemented on mandibu-lar molars. RPE was set and cemented and parents instructed to activate once every other day, and to return in one month. After two months of RPE activations, RPFM was adjusted and parents instructed in its use. (Figs. 9,10,11) Brackets were also bonded on the mandibu-lar teeth. (Figs. 12 &13) After two months of orthodontic therapy, the anterior crossbite is corrected and the mandibular brackets were removed. Patient's behavior deteriorated on and off during adjustment visits but the parents presence in the room helped with calming her down. After 7 months, the RPE was kept as a retention device and the RPFM use of 18 to 22 hours a day was suspended and used only at night. (Fig. 14) After 8 months of orthodontic treatment and during a dental appointment that included seda-tion, an impression with upper bands was taken to allow for fabri-cation of a fixed retention appli-ance. Once fabricated, the appliance was cemented to allow patient to continue using RPFM at home and always while sleeping. This would allow development of the maxillary arch in a forward and downward direction. Twenty-one months later, RPFM use was still encouraged and continued being used during sleep-ing hours. At 8.5 years of age, due to prolonged retention of tooth #D, tooth #7 erupted in crossbite. The patient was taught to use a tongue blade while sitting down, to encour-age proper eruption correcting the 26 Spring 2021 JAOS
Journal of the American Orthodontic Society Spring 2021: Page 26