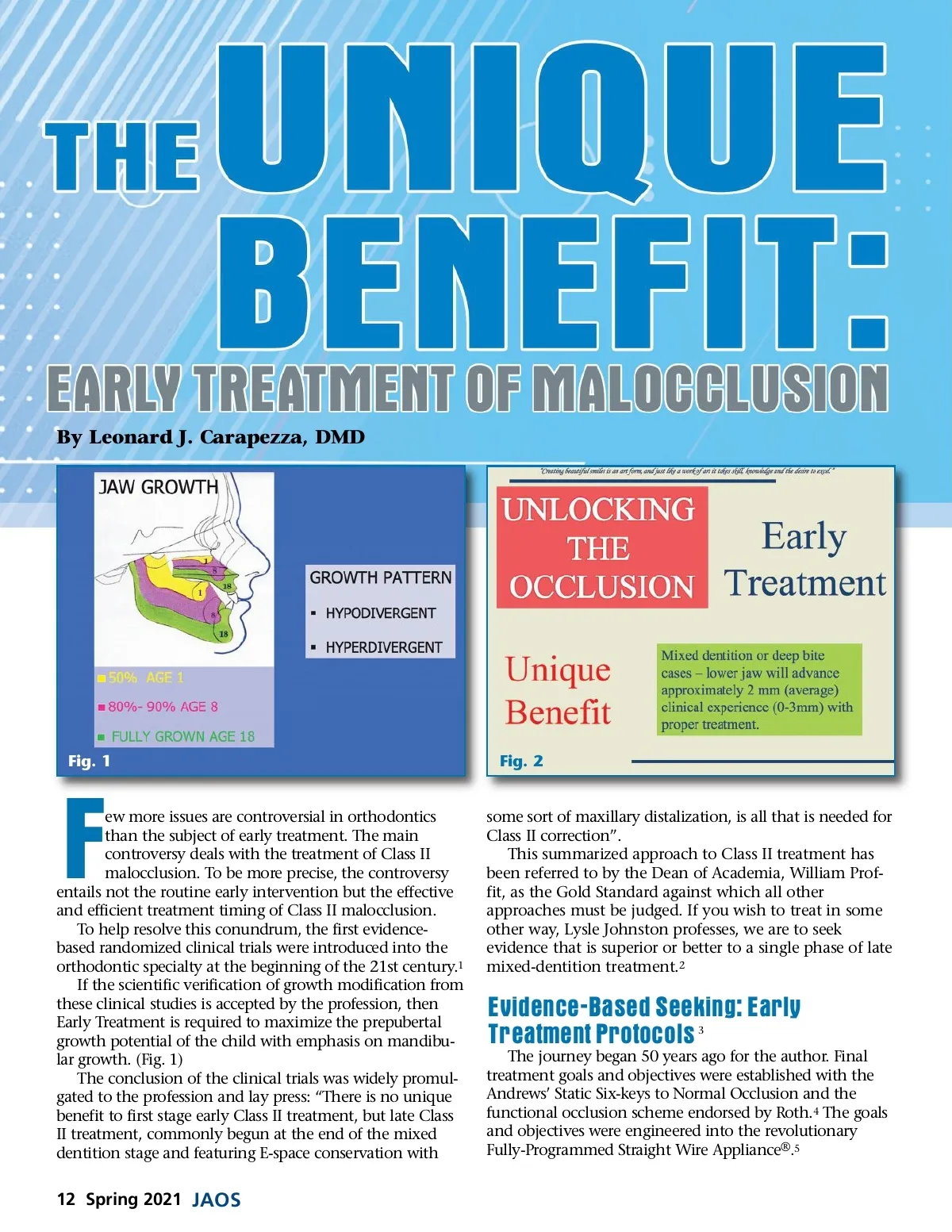
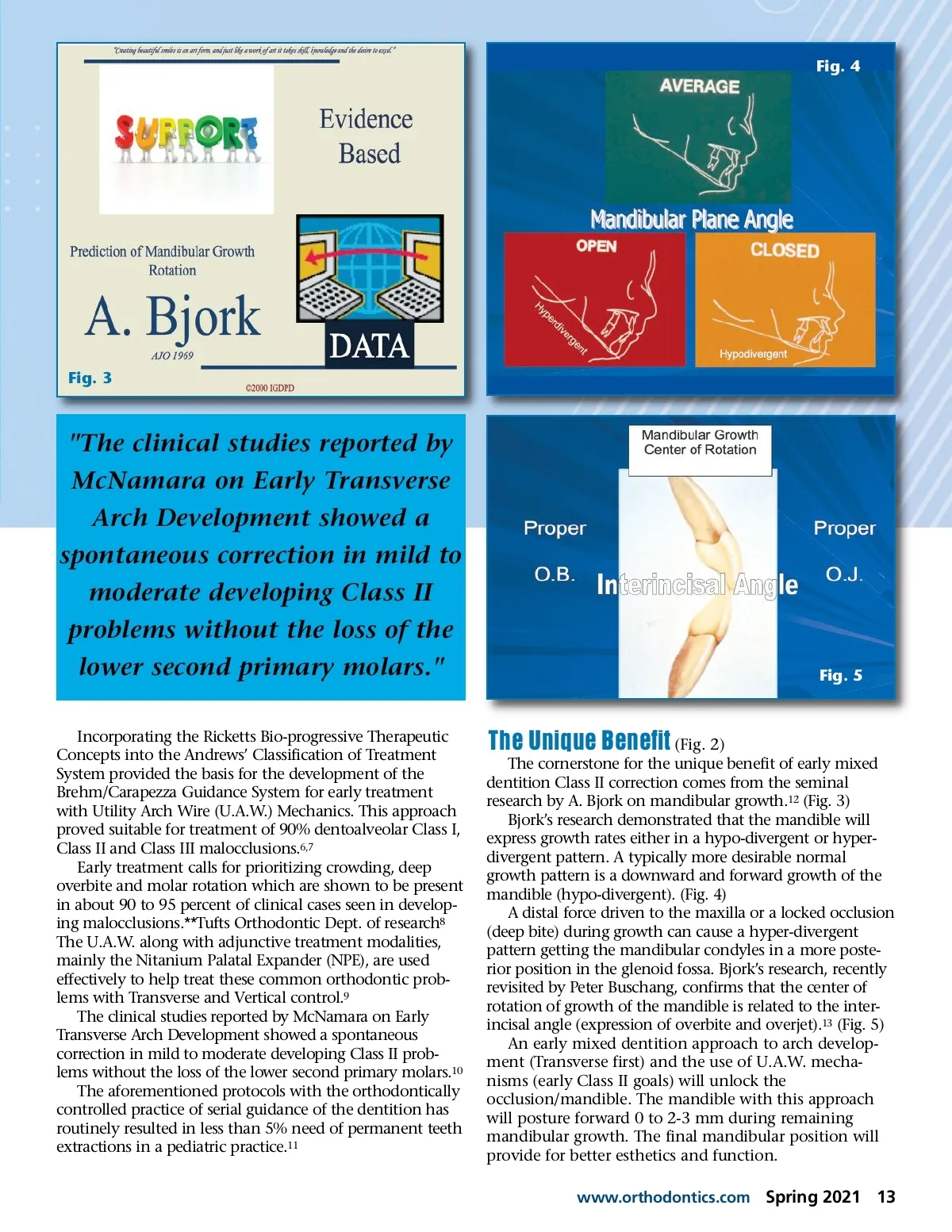
By Leonard J. Carapezza, DMD Fig. 1 Fig. 2 ew more issues are controversial in orthodontics than the subject of early treatment. The main controversy deals with the treatment of Class II malocclusion. To be more precise, the controversy entails not the routine early intervention but the effective and efficient treatment timing of Class II malocclusion. To help resolve this conundrum, the first evidence-based randomized clinical trials were introduced into the orthodontic specialty at the beginning of the 21st century. 1 If the scientific verification of growth modification from these clinical studies is accepted by the profession, then Early Treatment is required to maximize the prepubertal growth potential of the child with emphasis on mandibu-lar growth. (Fig. 1) The conclusion of the clinical trials was widely promul-gated to the profession and lay press: “There is no unique benefit to first stage early Class II treatment, but late Class II treatment, commonly begun at the end of the mixed dentition stage and featuring E-space conservation with F some sort of maxillary distalization, is all that is needed for Class II correction”. This summarized approach to Class II treatment has been referred to by the Dean of Academia, William Prof-fit, as the Gold Standard against which all other approaches must be judged. If you wish to treat in some other way, Lysle Johnston professes, we are to seek evidence that is superior or better to a single phase of late mixed-dentition treatment. 2 Evidence-Based Seeking: Early Treatment Protocols 3 The journey began 50 years ago for the author. Final treatment goals and objectives were established with the Andrews’ Static Six-keys to Normal Occlusion and the functional occlusion scheme endorsed by Roth. 4 The goals and objectives were engineered into the revolutionary Fully-Programmed Straight Wire Appliance ® . 5 12 Spring 2021 JAOS
Journal of the American Orthodontic Society Spring 2021: Page 12