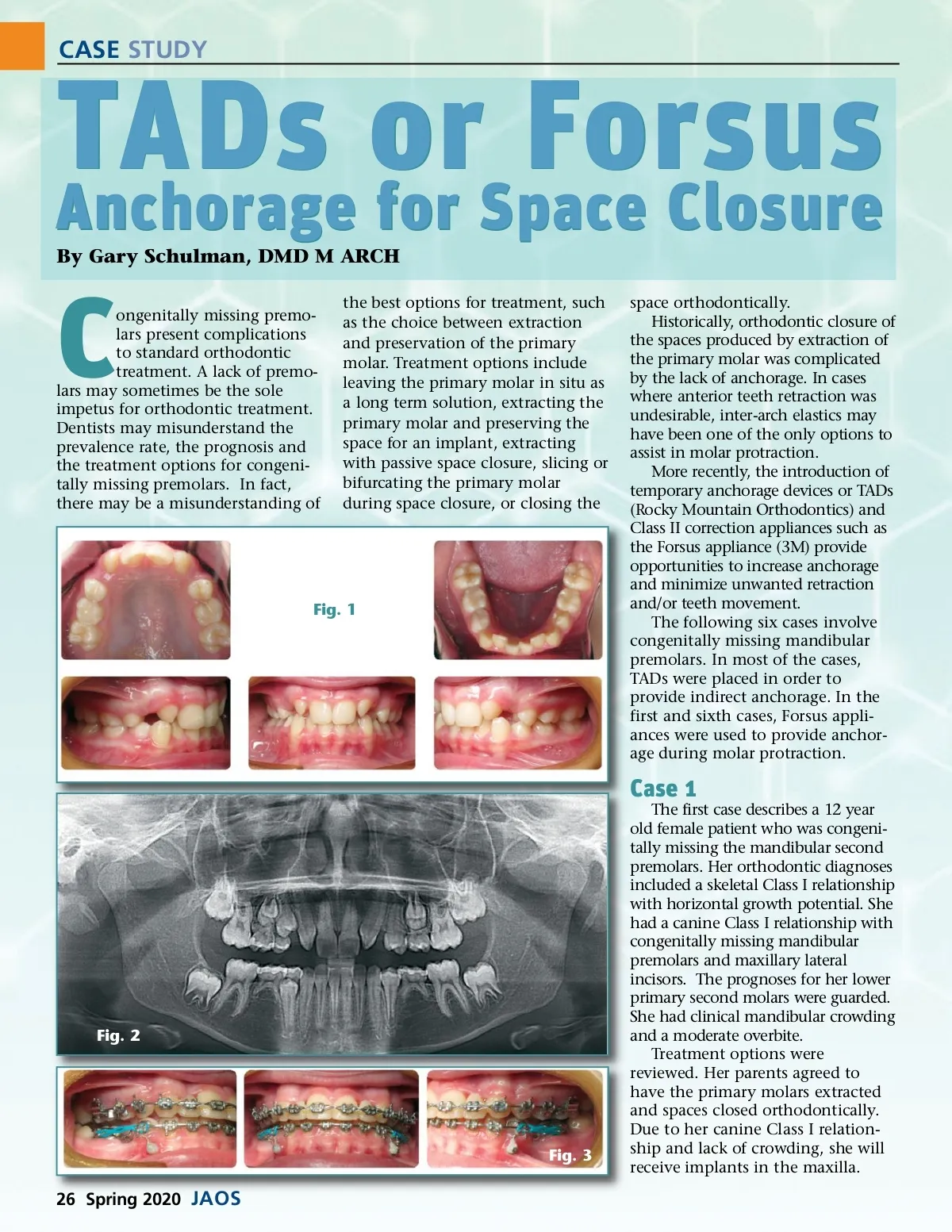
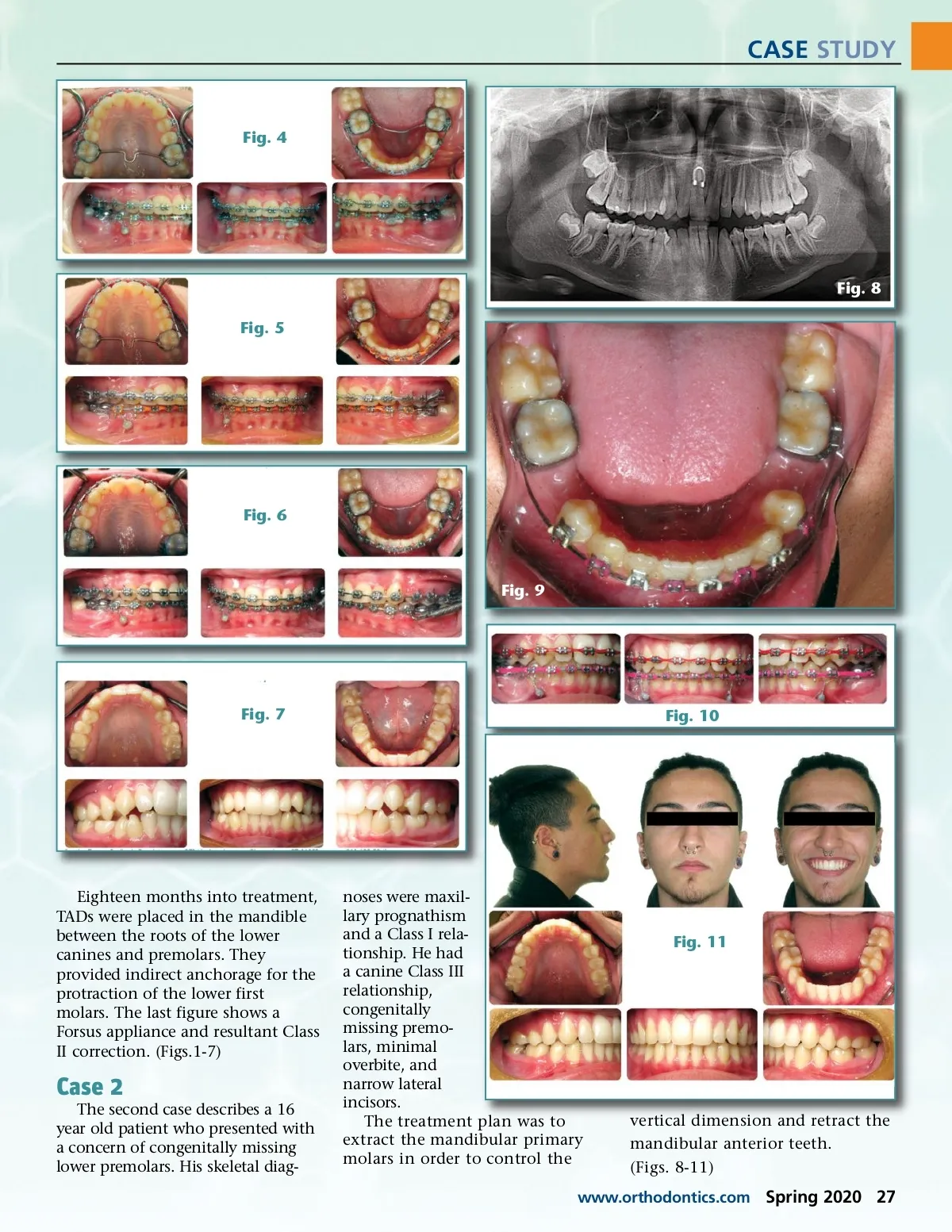
CASE STUDY TADs or Forsus Anchorage for Space Closure By Gary Schulman, DMD M ARCH C ongenitally missing premo-lars present complications to standard orthodontic treatment. A lack of premo-lars may sometimes be the sole impetus for orthodontic treatment. Dentists may misunderstand the prevalence rate, the prognosis and the treatment options for congeni-tally missing premolars. In fact, there may be a misunderstanding of the best options for treatment, such as the choice between extraction and preservation of the primary molar. Treatment options include leaving the primary molar in situ as a long term solution, extracting the primary molar and preserving the space for an implant, extracting with passive space closure, slicing or bifurcating the primary molar during space closure, or closing the Fig. 1 space orthodontically. Historically, orthodontic closure of the spaces produced by extraction of the primary molar was complicated by the lack of anchorage. In cases where anterior teeth retraction was undesirable, inter-arch elastics may have been one of the only options to assist in molar protraction. More recently, the introduction of temporary anchorage devices or TADs (Rocky Mountain Orthodontics) and Class II correction appliances such as the Forsus appliance (3M) provide opportunities to increase anchorage and minimize unwanted retraction and/or teeth movement. The following six cases involve congenitally missing mandibular premolars. In most of the cases, TADs were placed in order to provide indirect anchorage. In the first and sixth cases, Forsus appli-ances were used to provide anchor-age during molar protraction. Case 1 The first case describes a 12 year old female patient who was congeni-tally missing the mandibular second premolars. Her orthodontic diagnoses included a skeletal Class I relationship with horizontal growth potential. She had a canine Class I relationship with congenitally missing mandibular premolars and maxillary lateral incisors. The prognoses for her lower primary second molars were guarded. She had clinical mandibular crowding and a moderate overbite. Treatment options were reviewed. Her parents agreed to have the primary molars extracted and spaces closed orthodontically. Due to her canine Class I relation-ship and lack of crowding, she will receive implants in the maxilla. Fig. 2 Fig. 3 26 Spring 2020 JAOS
Journal of the American Orthodontic Society Spring 2020: Page 26