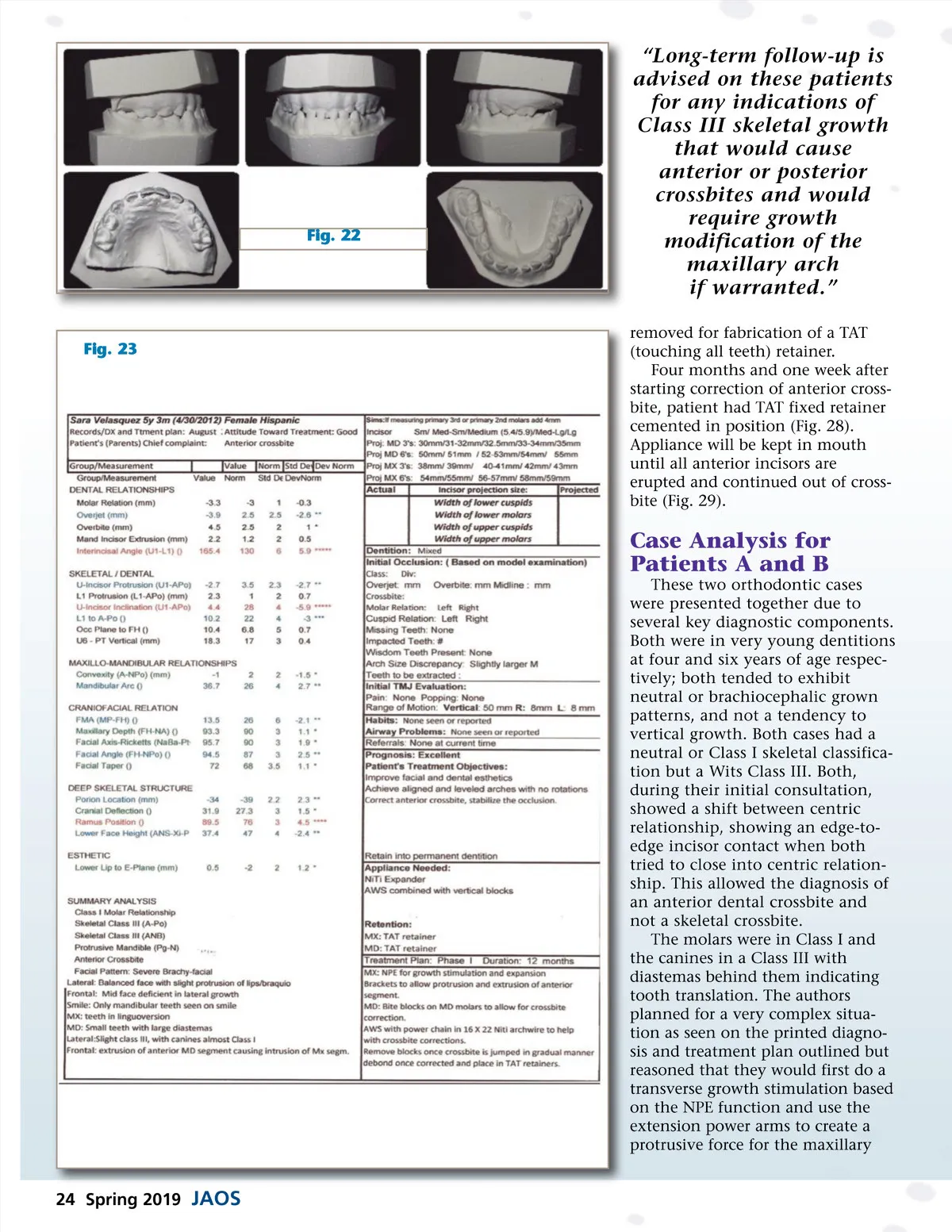
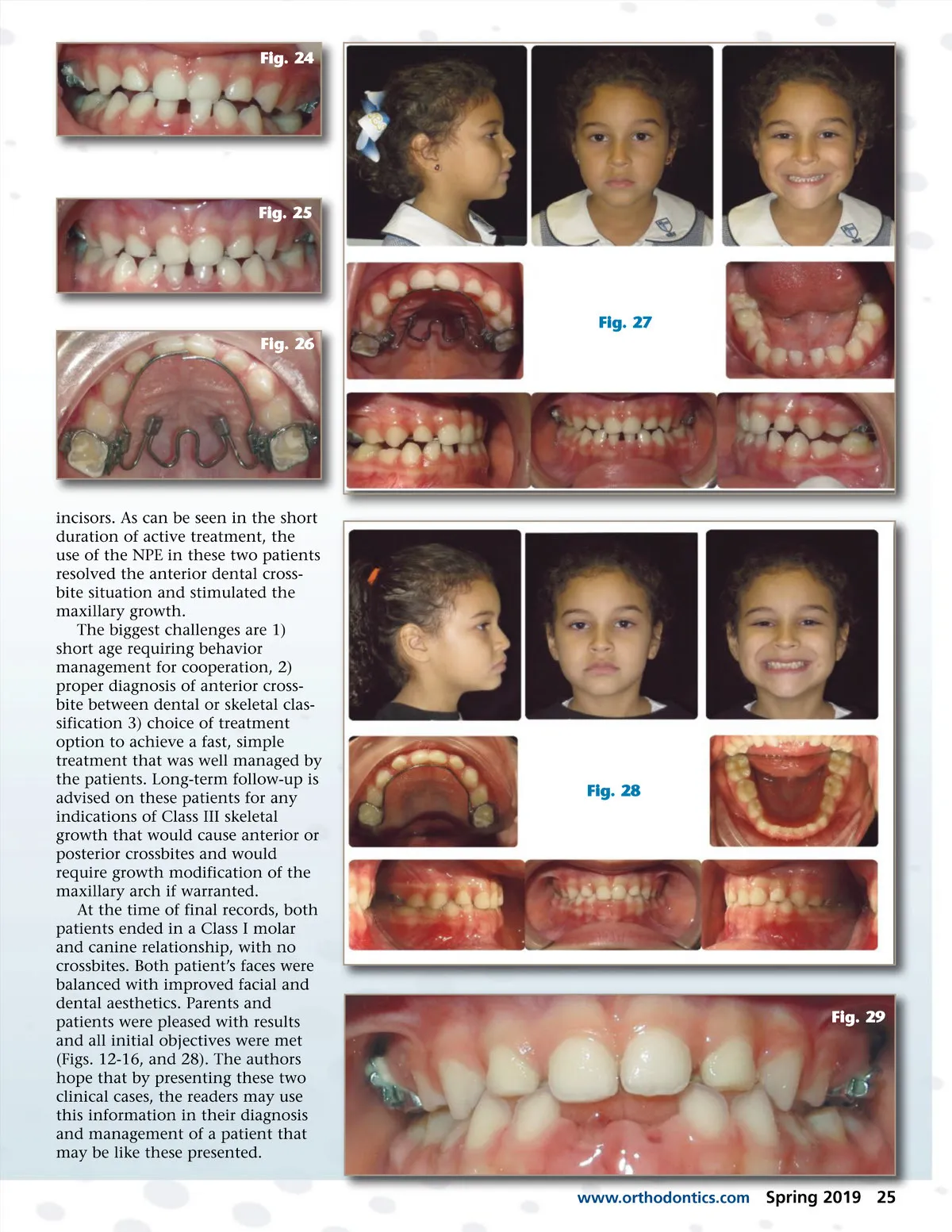
Fig. 22 “Long-term follow-up is advised on these patients for any indications of Class III skeletal growth that would cause anterior or posterior crossbites and would require growth modification of the maxillary arch if warranted.” removed for fabrication of a TAT (touching all teeth) retainer. Four months and one week after starting correction of anterior cross-bite, patient had TAT fixed retainer cemented in position (Fig. 28). Appliance will be kept in mouth until all anterior incisors are erupted and continued out of cross-bite (Fig. 29). Fig. 23 Case Analysis for Patients A and B These two orthodontic cases were presented together due to several key diagnostic components. Both were in very young dentitions at four and six years of age respec-tively; both tended to exhibit neutral or brachiocephalic grown patterns, and not a tendency to vertical growth. Both cases had a neutral or Class I skeletal classifica-tion but a Wits Class III. Both, during their initial consultation, showed a shift between centric relationship, showing an edge-to-edge incisor contact when both tried to close into centric relation-ship. This allowed the diagnosis of an anterior dental crossbite and not a skeletal crossbite. The molars were in Class I and the canines in a Class III with diastemas behind them indicating tooth translation. The authors planned for a very complex situa-tion as seen on the printed diagno-sis and treatment plan outlined but reasoned that they would first do a transverse growth stimulation based on the NPE function and use the extension power arms to create a protrusive force for the maxillary 24 Spring 2019 JAOS
Journal of the American Orthodontic Society Spring 2019: Page 24