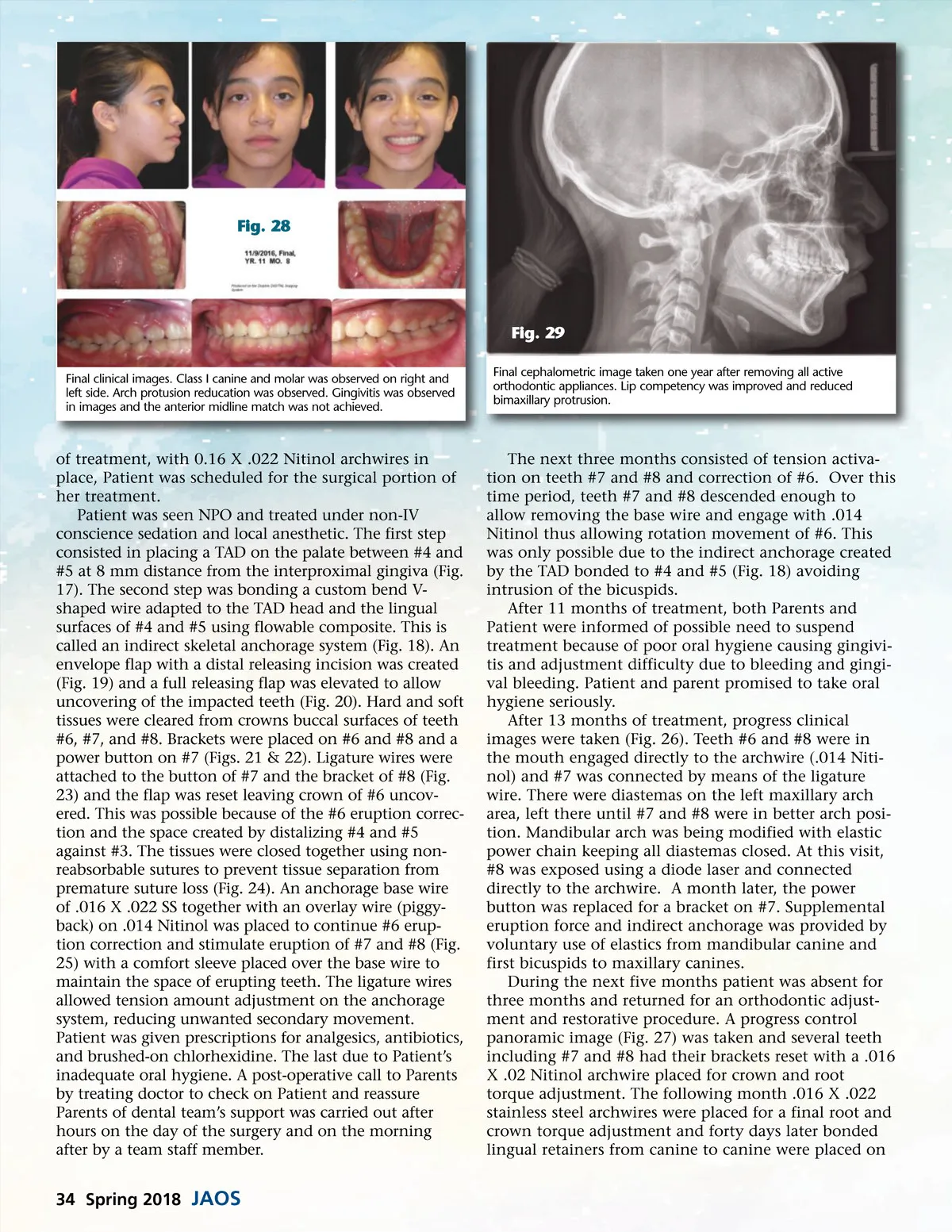
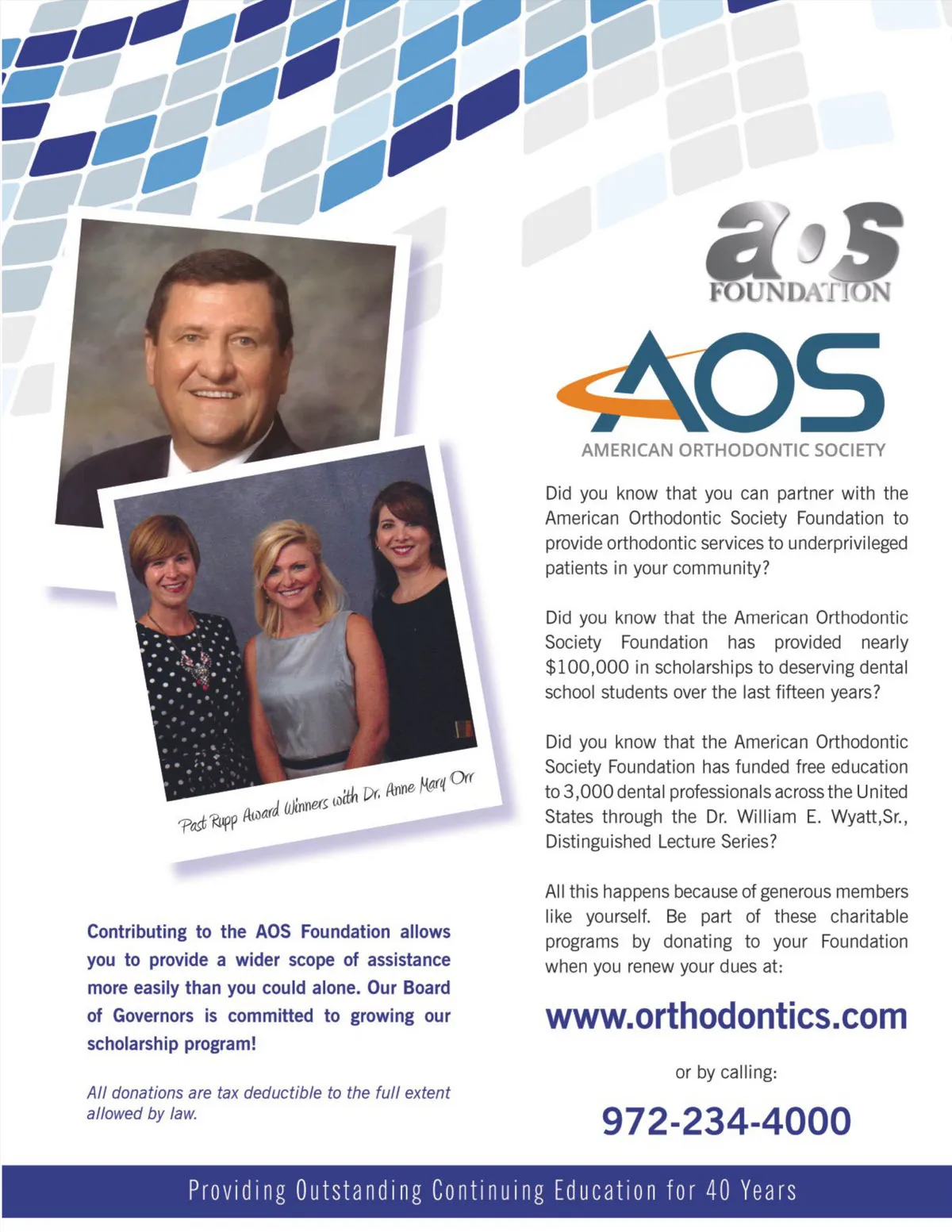
Fig. 28 Fig. 29 Final clinical images. Class I canine and molar was observed on right and left side. Arch protusion reducation was observed. Gingivitis was observed in images and the anterior midline match was not achieved. Final cephalometric image taken one year after removing all active orthodontic appliances. Lip competency was improved and reduced bimaxillary protrusion. of treatment, with 0.16 X .022 Nitinol archwires in place, Patient was scheduled for the surgical portion of her treatment. Patient was seen NPO and treated under non-IV conscience sedation and local anesthetic. The first step consisted in placing a TAD on the palate between #4 and #5 at 8 mm distance from the interproximal gingiva (Fig. 17). The second step was bonding a custom bend V-shaped wire adapted to the TAD head and the lingual surfaces of #4 and #5 using flowable composite. This is called an indirect skeletal anchorage system (Fig. 18). An envelope flap with a distal releasing incision was created (Fig. 19) and a full releasing flap was elevated to allow uncovering of the impacted teeth (Fig. 20). Hard and soft tissues were cleared from crowns buccal surfaces of teeth #6, #7, and #8. Brackets were placed on #6 and #8 and a power button on #7 (Figs. 21 & 22). Ligature wires were attached to the button of #7 and the bracket of #8 (Fig. 23) and the flap was reset leaving crown of #6 uncov-ered. This was possible because of the #6 eruption correc-tion and the space created by distalizing #4 and #5 against #3. The tissues were closed together using non-reabsorbable sutures to prevent tissue separation from premature suture loss (Fig. 24). An anchorage base wire of .016 X .022 SS together with an overlay wire (piggy-back) on .014 Nitinol was placed to continue #6 erup-tion correction and stimulate eruption of #7 and #8 (Fig. 25) with a comfort sleeve placed over the base wire to maintain the space of erupting teeth. The ligature wires allowed tension amount adjustment on the anchorage system, reducing unwanted secondary movement. Patient was given prescriptions for analgesics, antibiotics, and brushed-on chlorhexidine. The last due to Patient’s inadequate oral hygiene. A post-operative call to Parents by treating doctor to check on Patient and reassure Parents of dental team’s support was carried out after hours on the day of the surgery and on the morning after by a team staff member. The next three months consisted of tension activa-tion on teeth #7 and #8 and correction of #6. Over this time period, teeth #7 and #8 descended enough to allow removing the base wire and engage with .014 Nitinol thus allowing rotation movement of #6. This was only possible due to the indirect anchorage created by the TAD bonded to #4 and #5 (Fig. 18) avoiding intrusion of the bicuspids. After 11 months of treatment, both Parents and Patient were informed of possible need to suspend treatment because of poor oral hygiene causing gingivi-tis and adjustment difficulty due to bleeding and gingi-val bleeding. Patient and parent promised to take oral hygiene seriously. After 13 months of treatment, progress clinical images were taken (Fig. 26). Teeth #6 and #8 were in the mouth engaged directly to the archwire (.014 Niti-nol) and #7 was connected by means of the ligature wire. There were diastemas on the left maxillary arch area, left there until #7 and #8 were in better arch posi-tion. Mandibular arch was being modified with elastic power chain keeping all diastemas closed. At this visit, #8 was exposed using a diode laser and connected directly to the archwire. A month later, the power button was replaced for a bracket on #7. Supplemental eruption force and indirect anchorage was provided by voluntary use of elastics from mandibular canine and first bicuspids to maxillary canines. During the next five months patient was absent for three months and returned for an orthodontic adjust-ment and restorative procedure. A progress control panoramic image (Fig. 27) was taken and several teeth including #7 and #8 had their brackets reset with a .016 X .02 Nitinol archwire placed for crown and root torque adjustment. The following month .016 X .022 stainless steel archwires were placed for a final root and crown torque adjustment and forty days later bonded lingual retainers from canine to canine were placed on 34 Spring 2018 JAOS
Journal of the American Orthodontic Society Spring 2018: Page 34