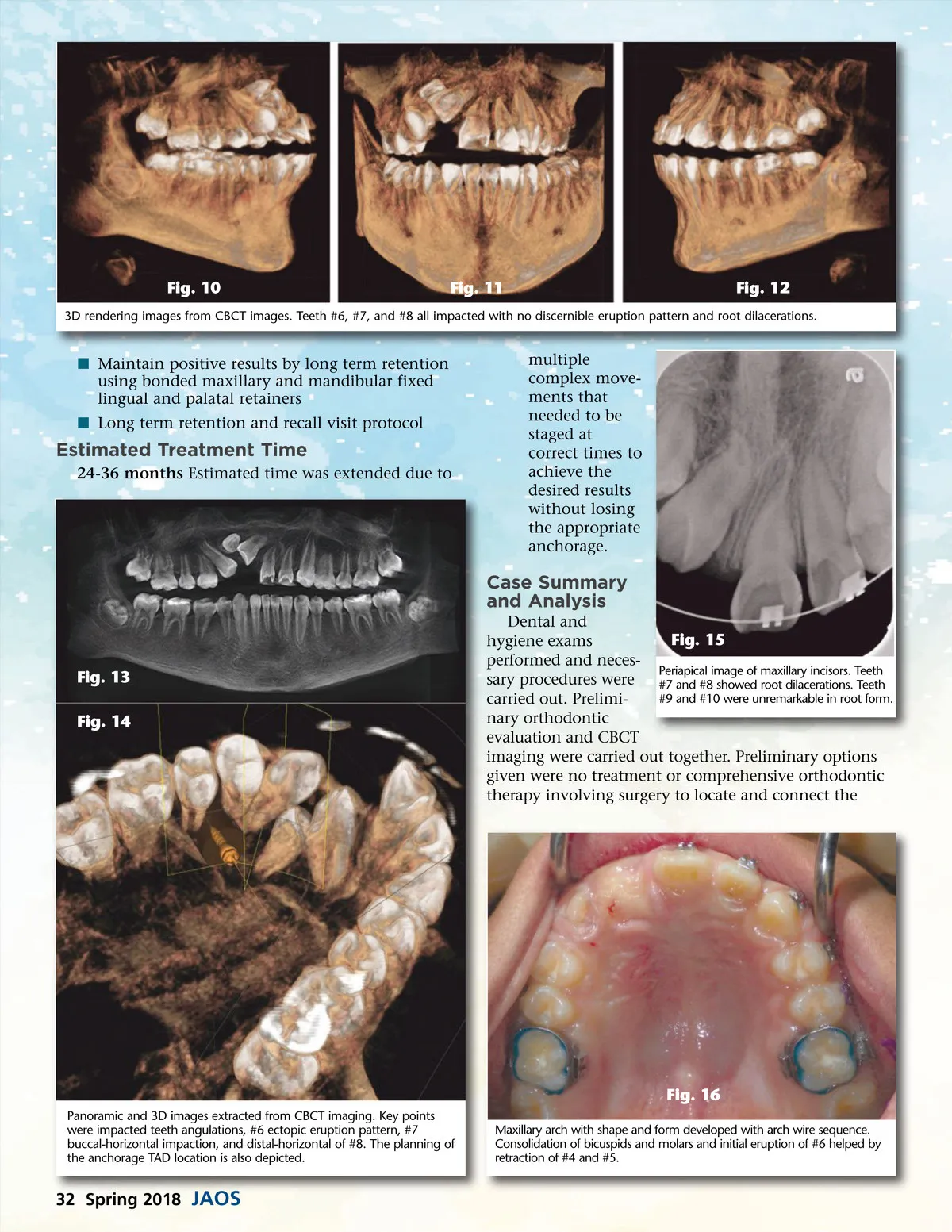
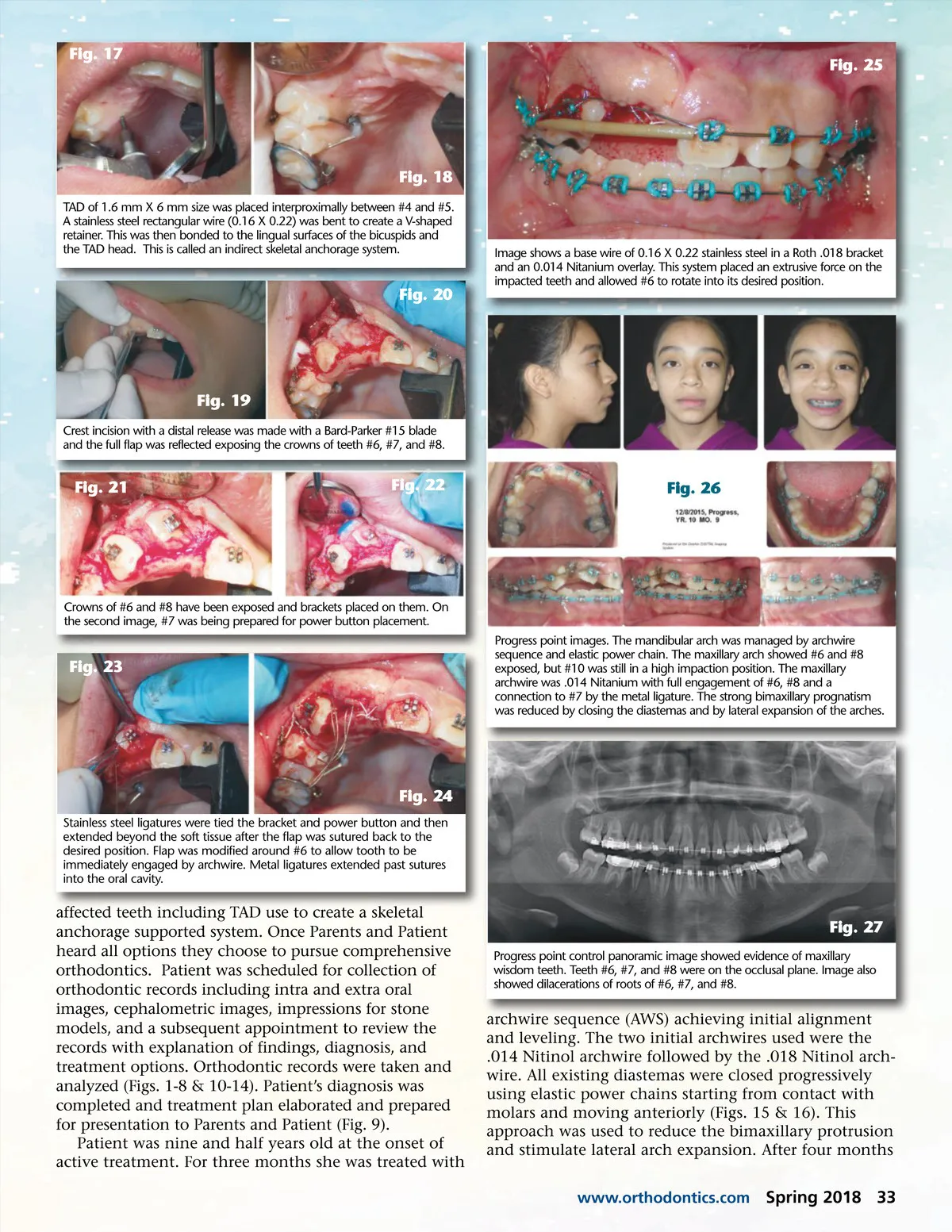
Fig. 17 Fig. 25 Fig. 18 TAD of 1.6 mm X 6 mm size was placed interproximally between #4 and #5. A stainless steel rectangular wire (0.16 X 0.22) was bent to create a V-shaped retainer. This was then bonded to the lingual surfaces of the bicuspids and the TAD head. This is called an indirect skeletal anchorage system. Image shows a base wire of 0.16 X 0.22 stainless steel in a Roth .018 bracket and an 0.014 Nitanium overlay. This system placed an extrusive force on the impacted teeth and allowed #6 to rotate into its desired position. Fig. 20 Fig. 19 Crest incision with a distal release was made with a Bard-Parker #15 blade and the full flap was reflected exposing the crowns of teeth #6, #7, and #8. Fig. 21 Fig. 22 Fig. 26 Crowns of #6 and #8 have been exposed and brackets placed on them. On the second image, #7 was being prepared for power button placement. Progress point images. The mandibular arch was managed by archwire sequence and elastic power chain. The maxillary arch showed #6 and #8 exposed, but #10 was still in a high impaction position. The maxillary archwire was .014 Nitanium with full engagement of #6, #8 and a connection to #7 by the metal ligature. The strong bimaxillary prognatism was reduced by closing the diastemas and by lateral expansion of the arches. Fig. 23 Fig. 24 Stainless steel ligatures were tied the bracket and power button and then extended beyond the soft tissue after the flap was sutured back to the desired position. Flap was modified around #6 to allow tooth to be immediately engaged by archwire. Metal ligatures extended past sutures into the oral cavity. affected teeth including TAD use to create a skeletal anchorage supported system. Once Parents and Patient heard all options they choose to pursue comprehensive orthodontics. Patient was scheduled for collection of orthodontic records including intra and extra oral images, cephalometric images, impressions for stone models, and a subsequent appointment to review the records with explanation of findings, diagnosis, and treatment options. Orthodontic records were taken and analyzed (Figs. 1-8 & 10-14). Patient’s diagnosis was completed and treatment plan elaborated and prepared for presentation to Parents and Patient (Fig. 9). Patient was nine and half years old at the onset of active treatment. For three months she was treated with Fig. 27 Progress point control panoramic image showed evidence of maxillary wisdom teeth. Teeth #6, #7, and #8 were on the occlusal plane. Image also showed dilacerations of roots of #6, #7, and #8. archwire sequence (AWS) achieving initial alignment and leveling. The two initial archwires used were the .014 Nitinol archwire followed by the .018 Nitinol arch-wire. All existing diastemas were closed progressively using elastic power chains starting from contact with molars and moving anteriorly (Figs. 15 & 16). This approach was used to reduce the bimaxillary protrusion and stimulate lateral arch expansion. After four months www.orthodontics.com Spring 2018 33
Journal of the American Orthodontic Society Spring 2018: Page 33