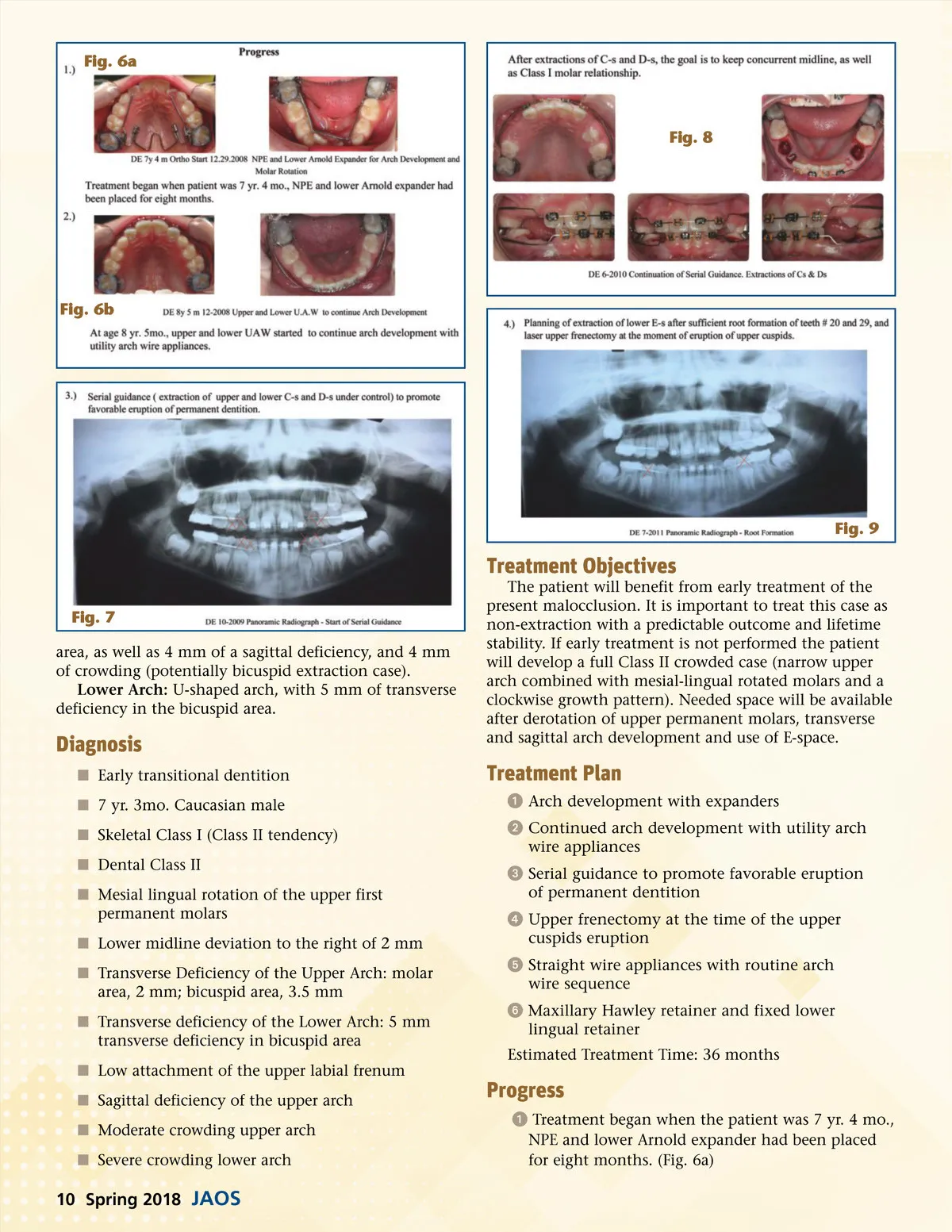
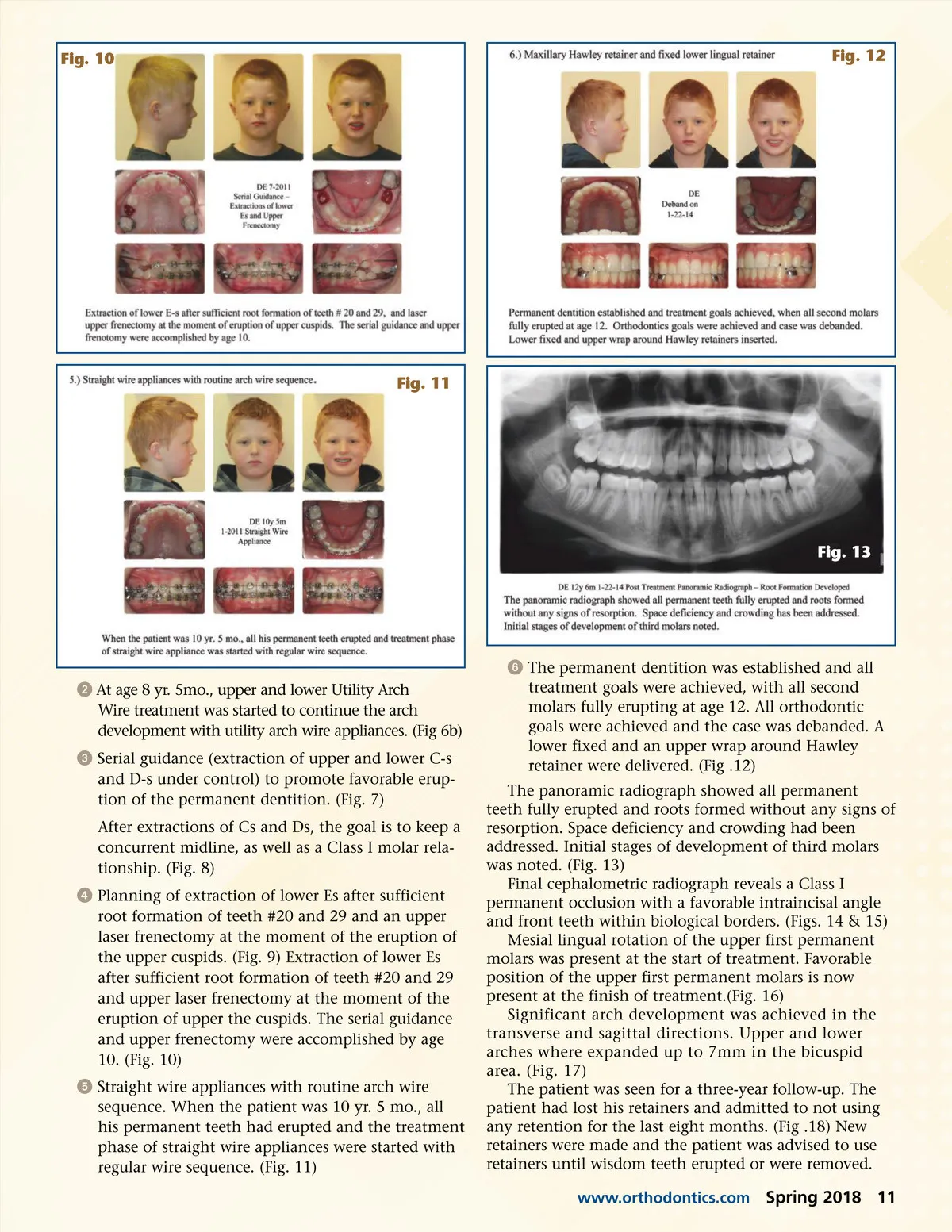
Fig. 6a Fig. 8 Fig. 6b Fig. 9 Treatment Objectives Fig. 7 area, as well as 4 mm of a sagittal deficiency, and 4 mm of crowding (potentially bicuspid extraction case). Lower Arch: U-shaped arch, with 5 mm of transverse deficiency in the bicuspid area. The patient will benefit from early treatment of the present malocclusion. It is important to treat this case as non-extraction with a predictable outcome and lifetime stability. If early treatment is not performed the patient will develop a full Class II crowded case (narrow upper arch combined with mesial-lingual rotated molars and a clockwise growth pattern). Needed space will be available after derotation of upper permanent molars, transverse and sagittal arch development and use of E-space. Diagnosis í Early transitional dentition í 7 yr. 3mo. Caucasian male í Skeletal Class I (Class II tendency) í Dental Class II í Mesial lingual rotation of the upper first permanent molars í Lower midline deviation to the right of 2 mm í Transverse Deficiency of the Upper Arch: molar area, 2 mm; bicuspid area, 3.5 mm í Transverse deficiency of the Lower Arch: 5 mm transverse deficiency in bicuspid area í Low attachment of the upper labial frenum í Sagittal deficiency of the upper arch í Moderate crowding upper arch í Severe crowding lower arch Treatment Plan ᕡ Arch development with expanders ᕢ Continued arch development with utility arch wire appliances ᕣ Serial guidance to promote favorable eruption of permanent dentition ᕤ Upper frenectomy at the time of the upper cuspids eruption ᕥ Straight wire appliances with routine arch wire sequence ᕦ Maxillary Hawley retainer and fixed lower lingual retainer Estimated Treatment Time: 36 months Progress ᕡ Treatment began when the patient was 7 yr. 4 mo., NPE and lower Arnold expander had been placed for eight months. (Fig. 6a) 10 Spring 2018 JAOS
Journal of the American Orthodontic Society Spring 2018: Page 10