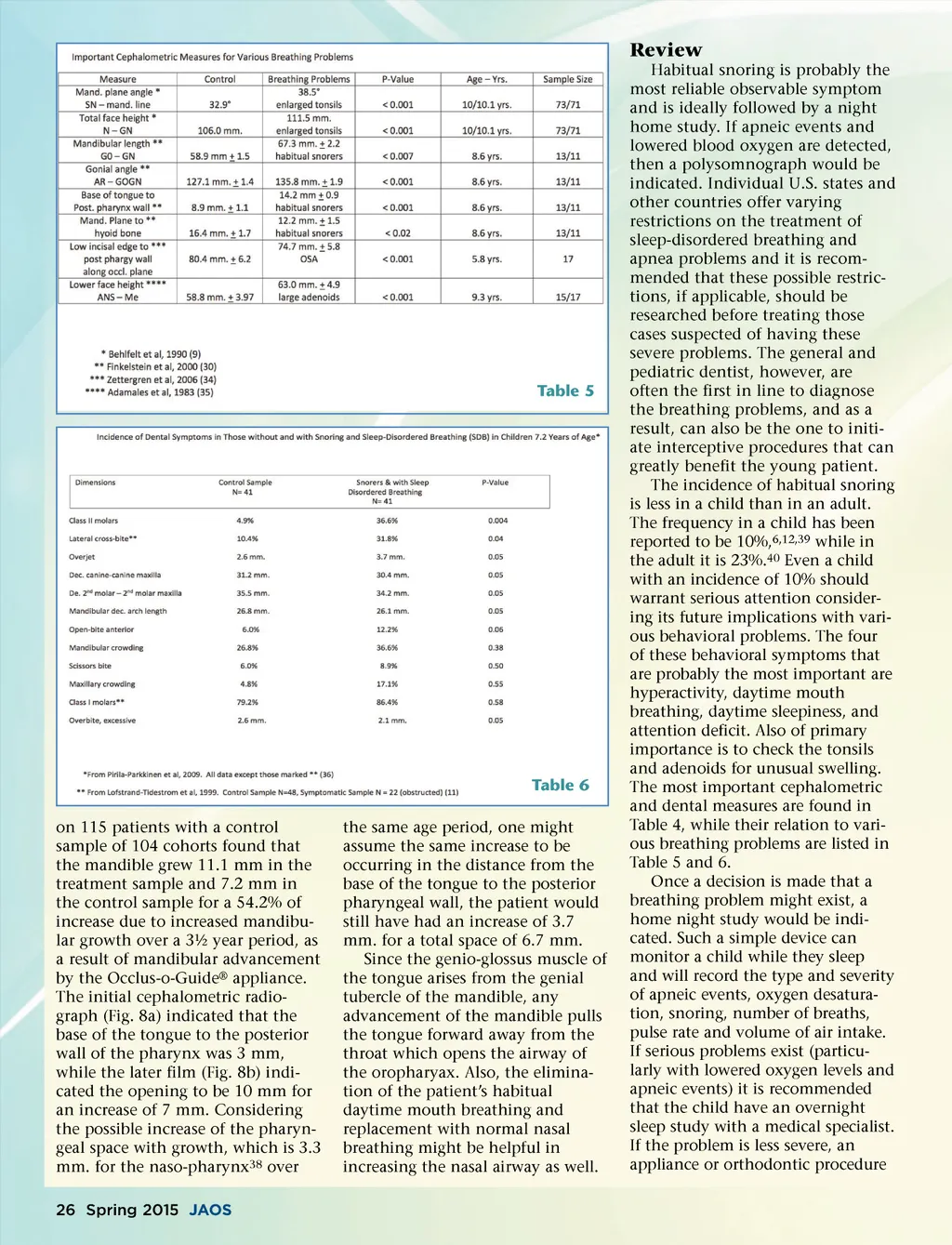
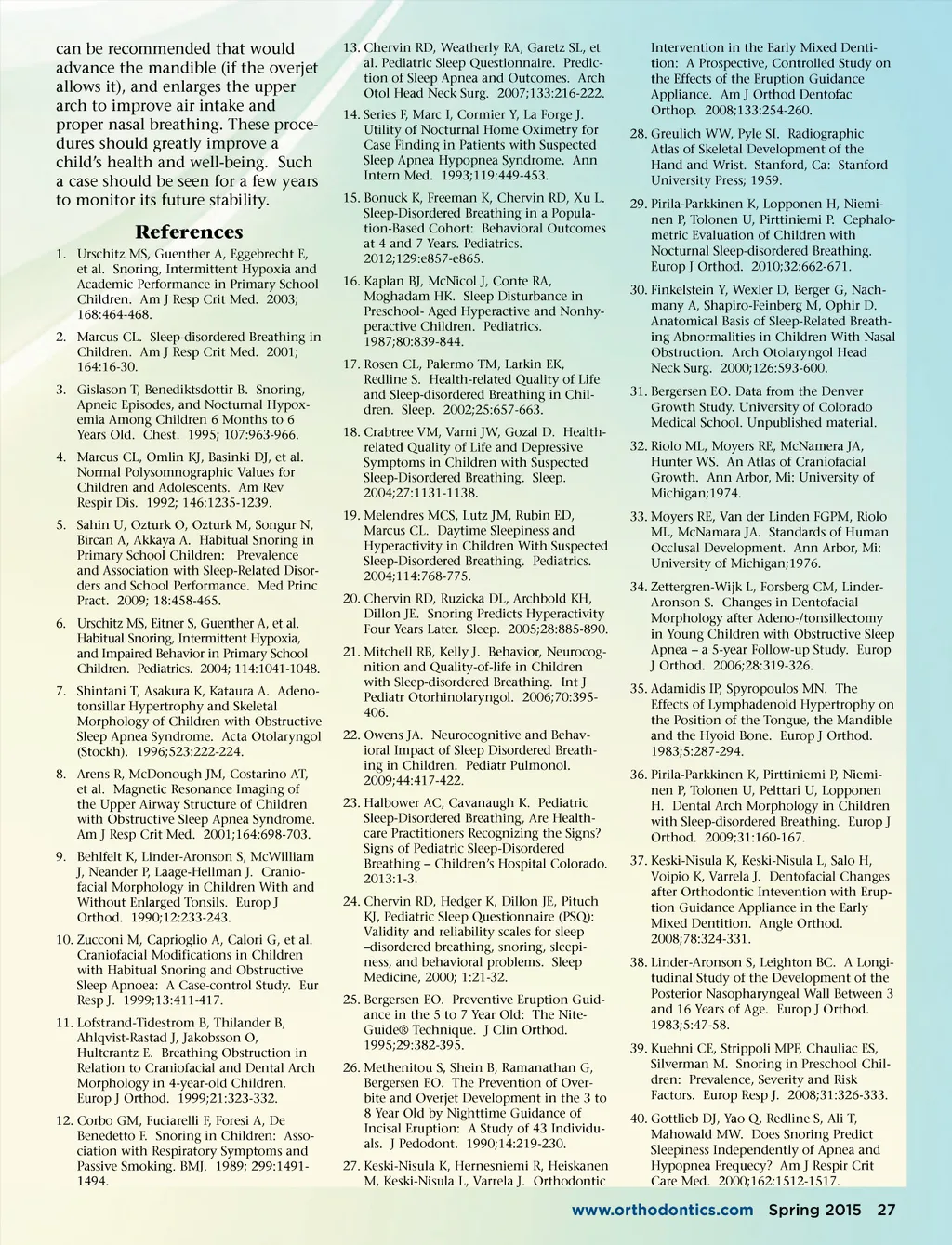
Review Habitual snoring is probably the most reliable observable symptom and is ideally followed by a night home study. If apneic events and lowered blood oxygen are detected, then a polysomnograph would be indicated. Individual U.S. states and other countries offer varying restrictions on the treatment of sleep-disordered breathing and apnea problems and it is recom-mended that these possible restric-tions, if applicable, should be researched before treating those cases suspected of having these severe problems. The general and pediatric dentist, however, are often the first in line to diagnose the breathing problems, and as a result, can also be the one to initi-ate interceptive procedures that can greatly benefit the young patient. The incidence of habitual snoring is less in a child than in an adult. The frequency in a child has been reported to be 10%, 6,12,39 while in the adult it is 23%. 40 Even a child with an incidence of 10% should warrant serious attention consider-ing its future implications with vari-ous behavioral problems. The four of these behavioral symptoms that are probably the most important are hyperactivity, daytime mouth breathing, daytime sleepiness, and attention deficit. Also of primary importance is to check the tonsils and adenoids for unusual swelling. The most important cephalometric and dental measures are found in Table 4, while their relation to vari-ous breathing problems are listed in Table 5 and 6. Once a decision is made that a breathing problem might exist, a home night study would be indi-cated. Such a simple device can monitor a child while they sleep and will record the type and severity of apneic events, oxygen desatura-tion, snoring, number of breaths, pulse rate and volume of air intake. If serious problems exist (particu-larly with lowered oxygen levels and apneic events) it is recommended that the child have an overnight sleep study with a medical specialist. If the problem is less severe, an appliance or orthodontic procedure Table 5 Table 6 on 115 patients with a control sample of 104 cohorts found that the mandible grew 11.1 mm in the treatment sample and 7.2 mm in the control sample for a 54.2% of increase due to increased mandibu-lar growth over a 3½ year period, as a result of mandibular advancement by the Occlus-o-Guide ® appliance. The initial cephalometric radio-graph (Fig. 8a) indicated that the base of the tongue to the posterior wall of the pharynx was 3 mm, while the later film (Fig. 8b) indi-cated the opening to be 10 mm for an increase of 7 mm. Considering the possible increase of the pharyn-geal space with growth, which is 3.3 mm. for the naso-pharynx 38 over 26 Spring 2015 JAOS the same age period, one might assume the same increase to be occurring in the distance from the base of the tongue to the posterior pharyngeal wall, the patient would still have had an increase of 3.7 mm. for a total space of 6.7 mm. Since the genio-glossus muscle of the tongue arises from the genial tubercle of the mandible, any advancement of the mandible pulls the tongue forward away from the throat which opens the airway of the oropharyax. Also, the elimina-tion of the patient’s habitual daytime mouth breathing and replacement with normal nasal breathing might be helpful in increasing the nasal airway as well.
Journal of the American Orthodontic Society Spring 2015: Page 26