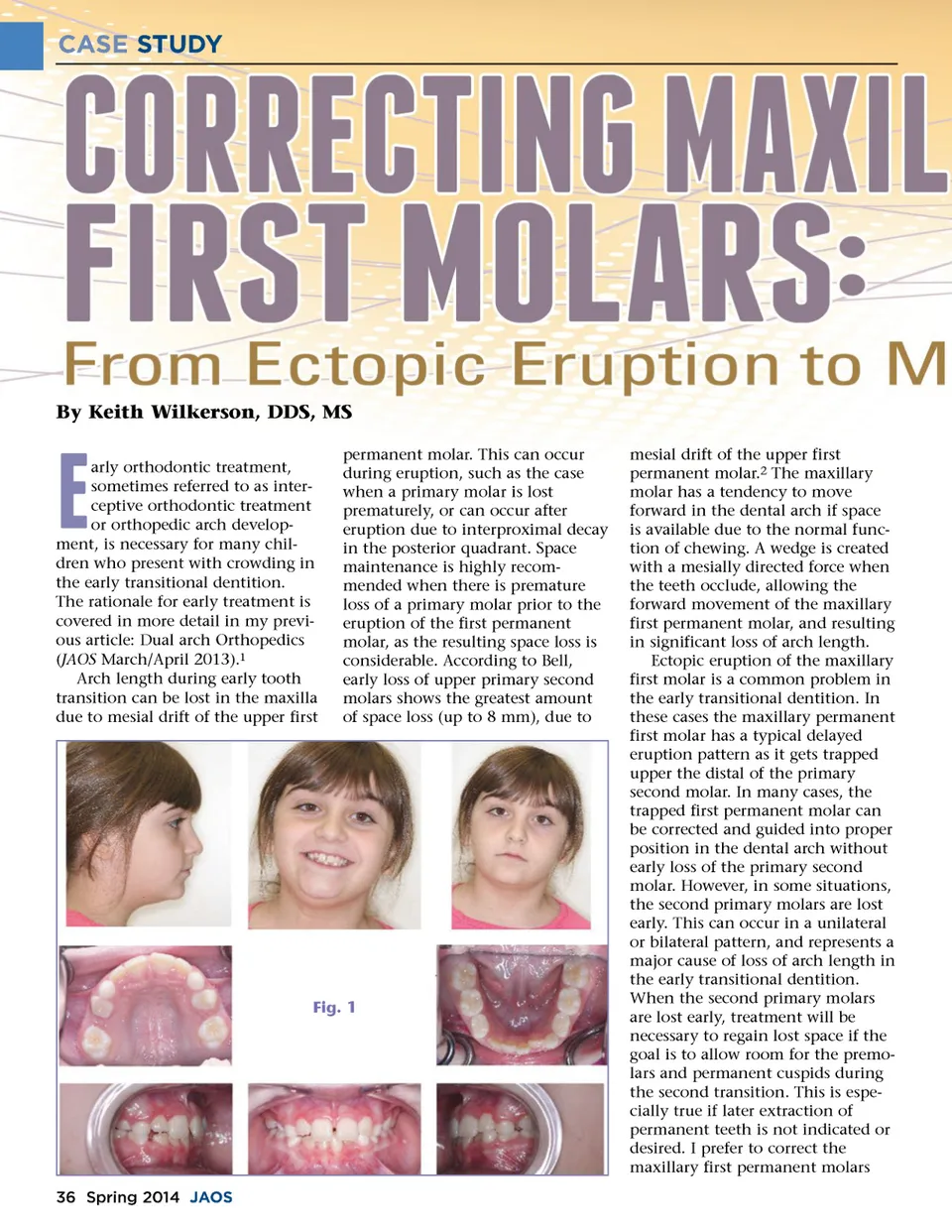
CASE STUDY By Keith Wilkerson, DDS, MS  arly orthodontic treatment, sometimes referred to as inter-ceptive orthodontic treatment or orthopedic arch develop-ment, is necessary for many chil-dren who present with crowding in the early transitional dentition. The rationale for early treatment is covered in more detail in my previ-ous article: Dual arch Orthopedics ( JAOS March/April 2013). 1 Arch length during early tooth transition can be lost in the maxilla due to mesial drift of the upper first permanent molar. This can occur during eruption, such as the case when a primary molar is lost prematurely, or can occur after eruption due to interproximal decay in the posterior quadrant. Space maintenance is highly recom-mended when there is premature loss of a primary molar prior to the eruption of the first permanent molar, as the resulting space loss is considerable. According to Bell, early loss of upper primary second molars shows the greatest amount of space loss (up to 8 mm), due to Fig. 1 mesial drift of the upper first permanent molar. 2 The maxillary molar has a tendency to move forward in the dental arch if space is available due to the normal func-tion of chewing. A wedge is created with a mesially directed force when the teeth occlude, allowing the forward movement of the maxillary first permanent molar, and resulting in significant loss of arch length. Ectopic eruption of the maxillary first molar is a common problem in the early transitional dentition. In these cases the maxillary permanent first molar has a typical delayed eruption pattern as it gets trapped upper the distal of the primary second molar. In many cases, the trapped first permanent molar can be corrected and guided into proper position in the dental arch without early loss of the primary second molar. However, in some situations, the second primary molars are lost early. This can occur in a unilateral or bilateral pattern, and represents a major cause of loss of arch length in the early transitional dentition. When the second primary molars are lost early, treatment will be necessary to regain lost space if the goal is to allow room for the premo-lars and permanent cuspids during the second transition. This is espe-cially true if later extraction of permanent teeth is not indicated or desired. I prefer to correct the maxillary first permanent molars 36 Spring 2014 JAOS
Journal of the American Orthodontic Society Spring 2014: Page 36