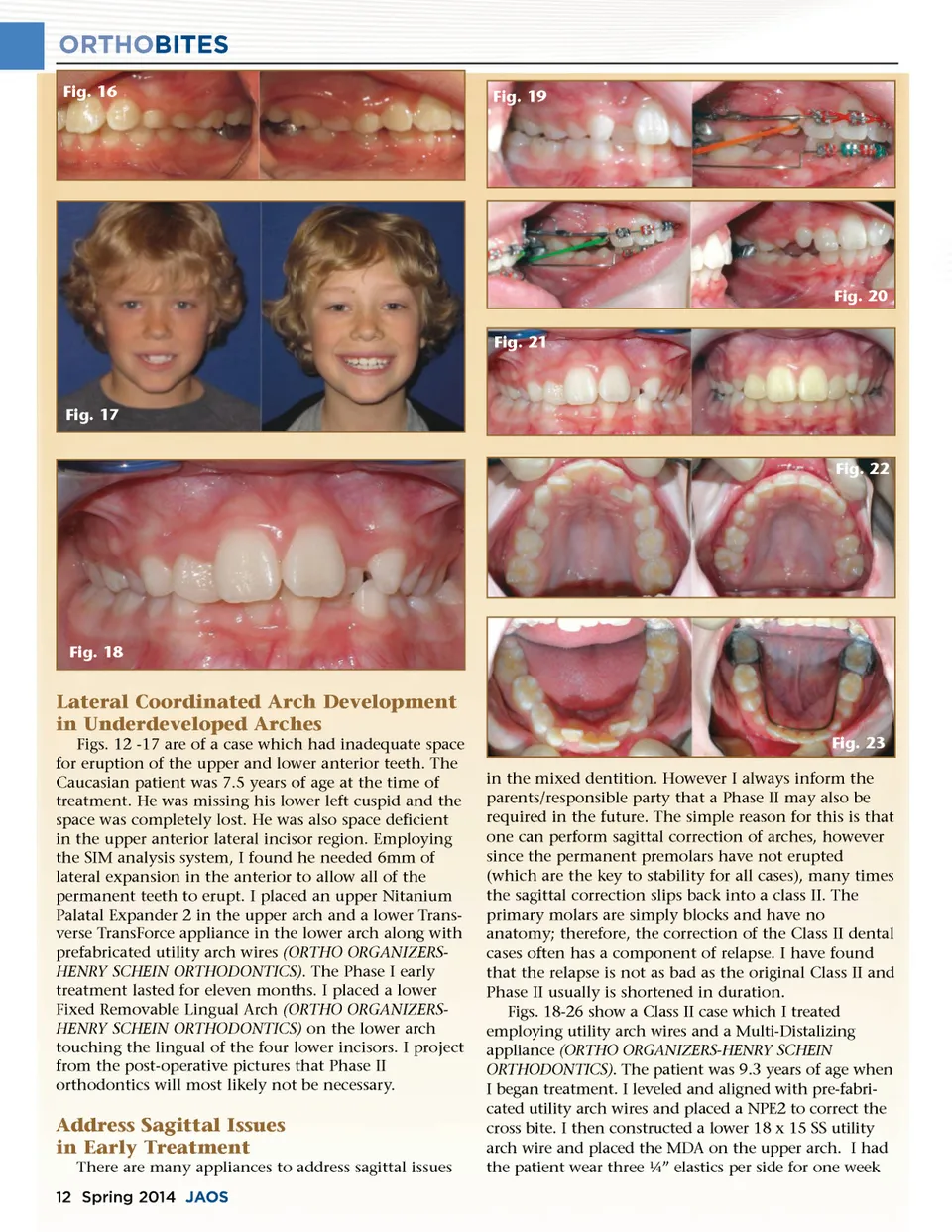
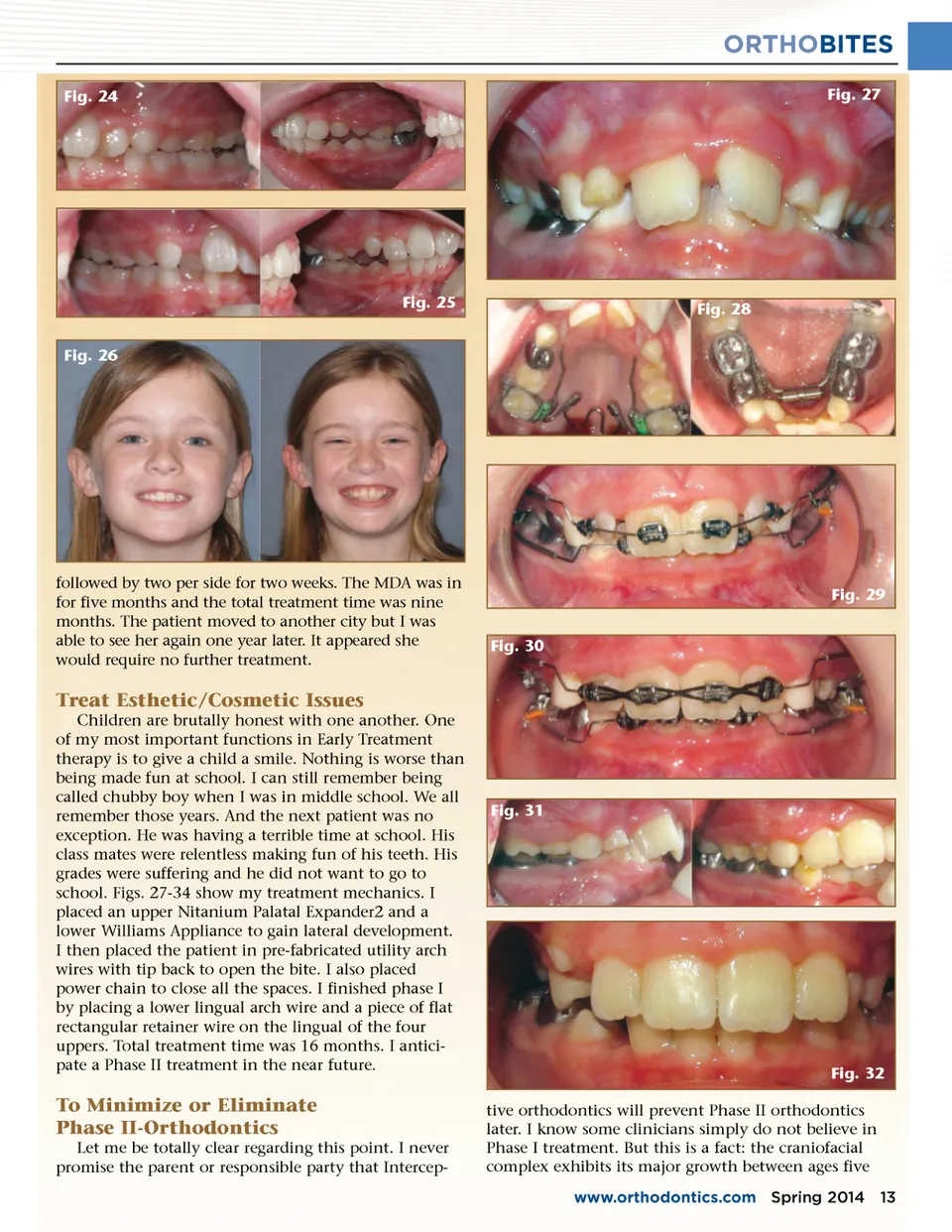
ORTHOBITES Fig. 24 Fig. 27 Fig. 25 Fig. 26 Fig. 28 followed by two per side for two weeks. The MDA was in for five months and the total treatment time was nine months. The patient moved to another city but I was able to see her again one year later. It appeared she would require no further treatment. Fig. 29 Fig. 30 Treat Esthetic/Cosmetic Issues Children are brutally honest with one another. One of my most important functions in Early Treatment therapy is to give a child a smile. Nothing is worse than being made fun at school. I can still remember being called chubby boy when I was in middle school. We all remember those years. And the next patient was no exception. He was having a terrible time at school. His class mates were relentless making fun of his teeth. His grades were suffering and he did not want to go to school. Figs. 27-34 show my treatment mechanics. I placed an upper Nitanium Palatal Expander2 and a lower Williams Appliance to gain lateral development. I then placed the patient in pre-fabricated utility arch wires with tip back to open the bite. I also placed power chain to close all the spaces. I finished phase I by placing a lower lingual arch wire and a piece of flat rectangular retainer wire on the lingual of the four uppers. Total treatment time was 16 months. I antici-pate a Phase II treatment in the near future. Fig. 31 Fig. 32 tive orthodontics will prevent Phase II orthodontics later. I know some clinicians simply do not believe in Phase I treatment. But this is a fact: the craniofacial complex exhibits its major growth between ages five www.orthodontics.com Spring 2014 13 To Minimize or Eliminate Phase II-Orthodontics Let me be totally clear regarding this point. I never promise the parent or responsible party that Intercep-
Journal of the American Orthodontic Society Spring 2014: Page 13