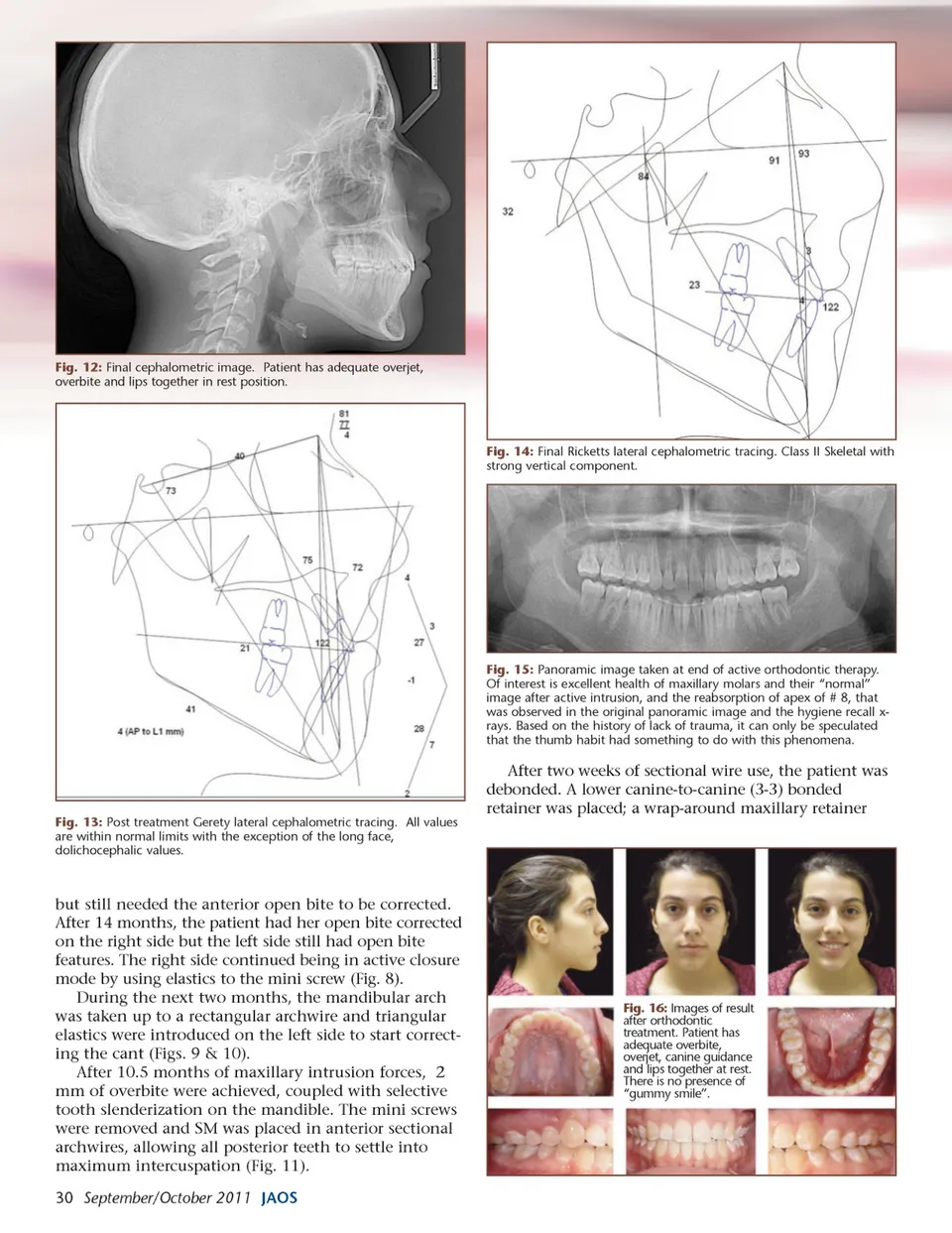
Fig. 12: Final cephalometric image. Patient has adequate overjet, overbite and lips together in rest position. Fig. 14: Final Ricketts lateral cephalometric tracing. Class II Skeletal with strong vertical component. Fig. 15: Panoramic image taken at end of active orthodontic therapy. Of interest is excellent health of maxillary molars and their “normal” image after active intrusion, and the reabsorption of apex of # 8, that was observed in the original panoramic image and the hygiene recall x-rays. Based on the history of lack of trauma, it can only be speculated that the thumb habit had something to do with this phenomena. After two weeks of sectional wire use, the patient was debonded. A lower canine-to-canine (3-3) bonded retainer was placed; a wrap-around maxillary retainer Fig. 13: Post treatment Gerety lateral cephalometric tracing. All values are within normal limits with the exception of the long face, dolichocephalic values. but still needed the anterior open bite to be corrected. After 14 months, the patient had her open bite corrected on the right side but the left side still had open bite features. The right side continued being in active closure mode by using elastics to the mini screw (Fig. 8). During the next two months, the mandibular arch was taken up to a rectangular archwire and triangular elastics were introduced on the left side to start correct-ing the cant (Figs. 9 & 10). After 10.5 months of maxillary intrusion forces, 2 mm of overbite were achieved, coupled with selective tooth slenderization on the mandible. The mini screws were removed and SM was placed in anterior sectional archwires, allowing all posterior teeth to settle into maximum intercuspation (Fig. 11). 30 September/October 2011 JAOS Fig. 16: Images of result after orthodontic treatment. Patient has adequate overbite, overjet, canine guidance and lips together at rest. There is no presence of “gummy smile”.
Journal of the American Orthodontic Society September-October 2011: Page 30