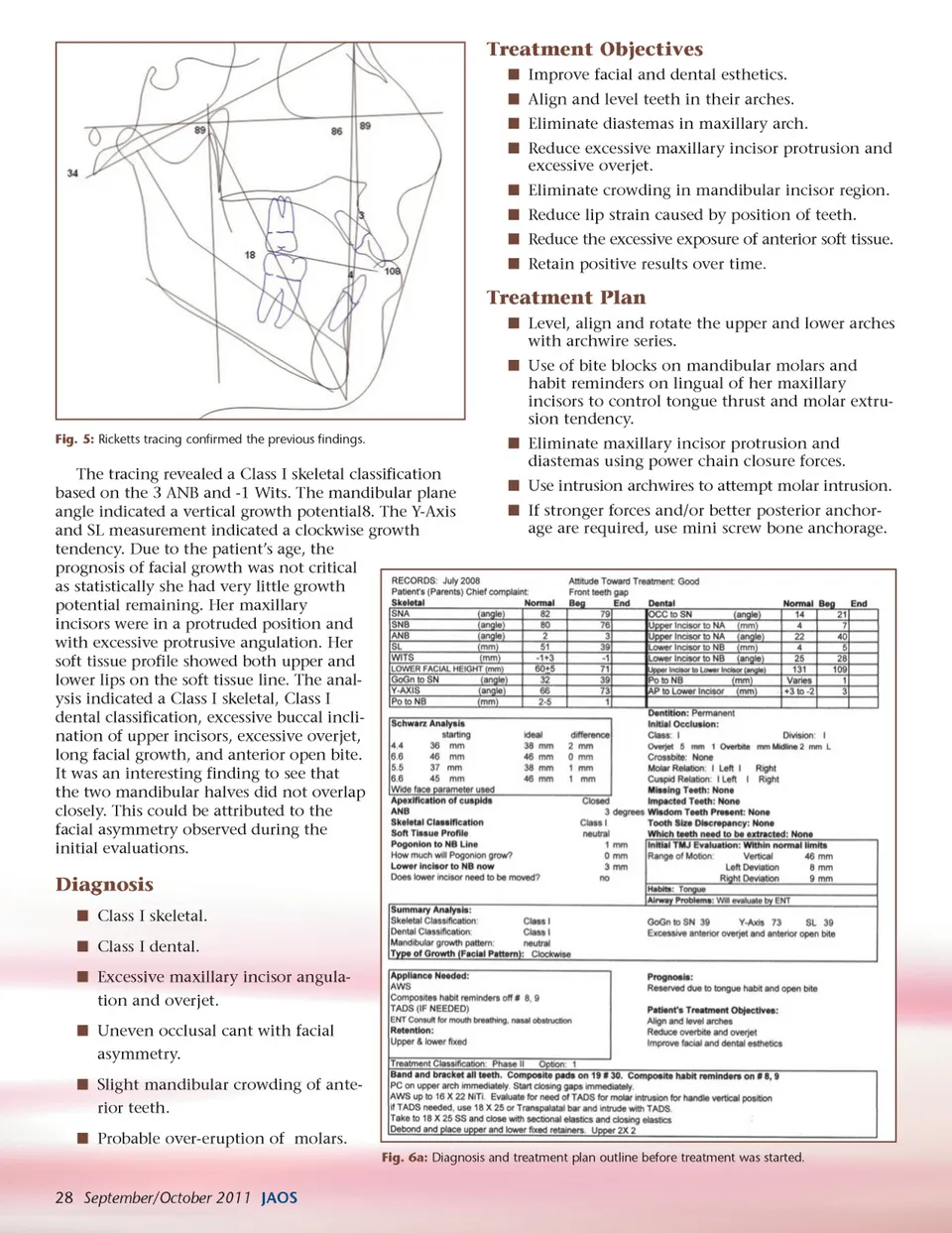
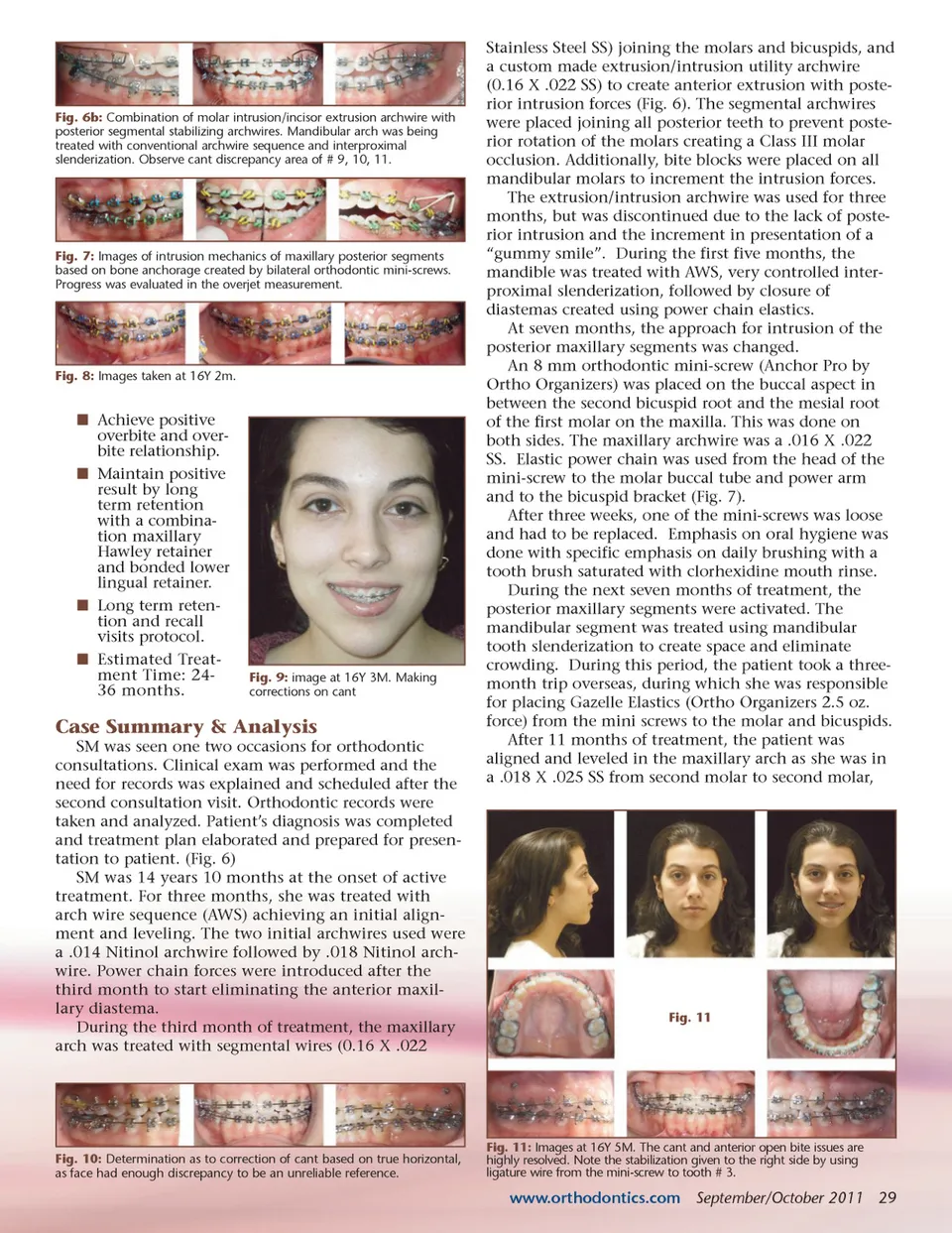
Treatment Objectives í Improve facial and dental esthetics. í Align and level teeth in their arches. í Eliminate diastemas in maxillary arch. í Reduce excessive maxillary incisor protrusion and excessive overjet. í Eliminate crowding in mandibular incisor region. í Reduce lip strain caused by position of teeth. í Reduce the excessive exposure of anterior soft tissue. í Retain positive results over time. Treatment Plan í Level, align and rotate the upper and lower arches with archwire series. í Use of bite blocks on mandibular molars and habit reminders on lingual of her maxillary incisors to control tongue thrust and molar extru-sion tendency. Fig. 5: Ricketts tracing confirmed the previous findings. The tracing revealed a Class I skeletal classification based on the 3 ANB and -1 Wits. The mandibular plane angle indicated a vertical growth potential8. The Y-Axis and SL measurement indicated a clockwise growth tendency. Due to the patient’s age, the prognosis of facial growth was not critical as statistically she had very little growth potential remaining. Her maxillary incisors were in a protruded position and with excessive protrusive angulation. Her soft tissue profile showed both upper and lower lips on the soft tissue line. The anal-ysis indicated a Class I skeletal, Class I dental classification, excessive buccal incli-nation of upper incisors, excessive overjet, long facial growth, and anterior open bite. It was an interesting finding to see that the two mandibular halves did not overlap closely. This could be attributed to the facial asymmetry observed during the initial evaluations. í Eliminate maxillary incisor protrusion and diastemas using power chain closure forces. í Use intrusion archwires to attempt molar intrusion. í If stronger forces and/or better posterior anchor-age are required, use mini screw bone anchorage. Diagnosis í Class I skeletal. í Class I dental. í Excessive maxillary incisor angula-tion and overjet. í Uneven occlusal cant with facial asymmetry. í Slight mandibular crowding of ante-rior teeth. í Probable over-eruption of molars. Fig. 6a: Diagnosis and treatment plan outline before treatment was started. 28 September/October 2011 JAOS
Journal of the American Orthodontic Society September-October 2011: Page 28