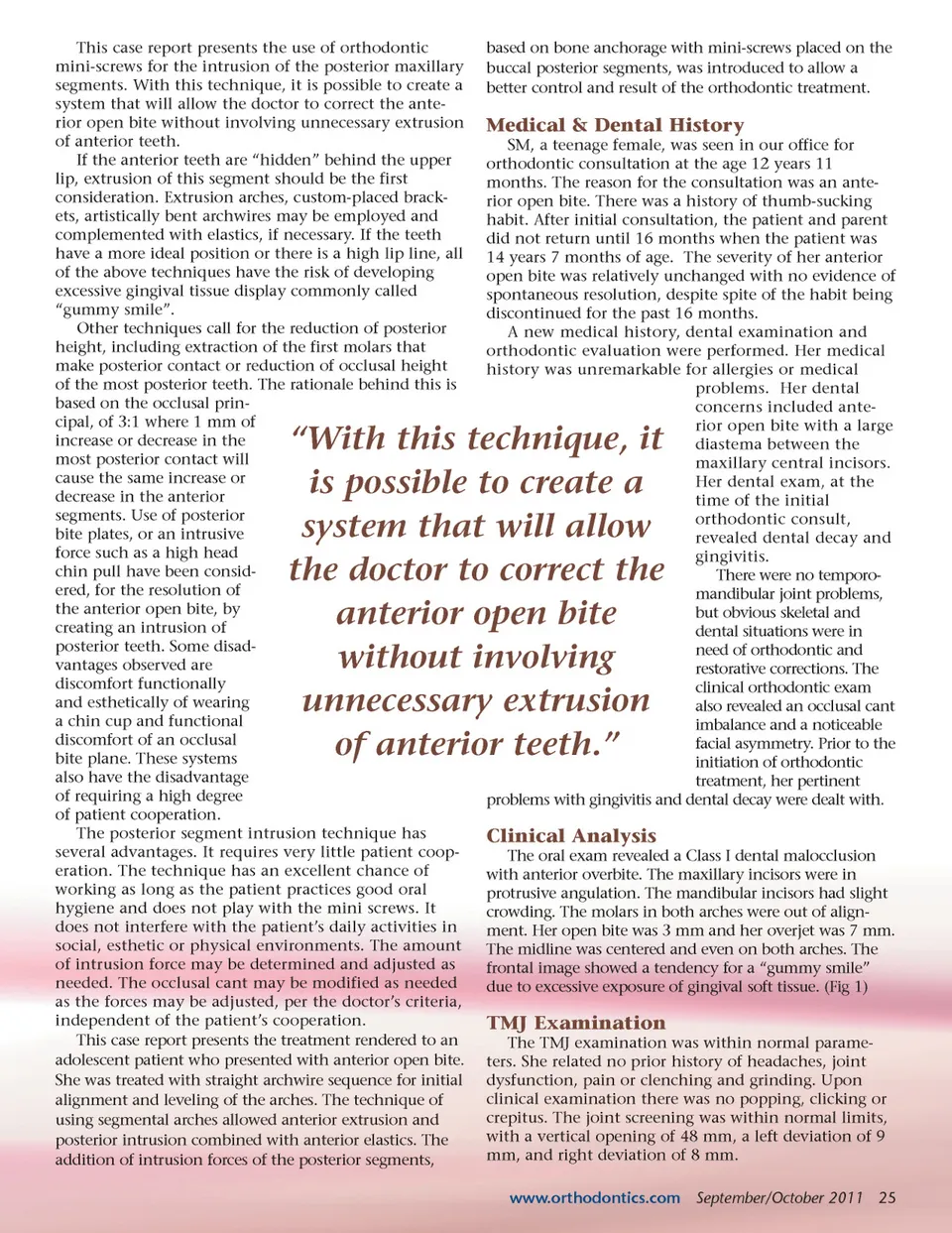
This case report presents the use of orthodontic mini-screws for the intrusion of the posterior maxillary segments. With this technique, it is possible to create a system that will allow the doctor to correct the ante-rior open bite without involving unnecessary extrusion of anterior teeth. If the anterior teeth are “hidden” behind the upper lip, extrusion of this segment should be the first consideration. Extrusion arches, custom-placed brack-ets, artistically bent archwires may be employed and complemented with elastics, if necessary. If the teeth have a more ideal position or there is a high lip line, all of the above techniques have the risk of developing excessive gingival tissue display commonly called “gummy smile”. Other techniques call for the reduction of posterior height, including extraction of the first molars that make posterior contact or reduction of occlusal height of the most posterior teeth. The rationale behind this is based on the occlusal prin-cipal, of 3:1 where 1 mm of increase or decrease in the most posterior contact will cause the same increase or decrease in the anterior segments. Use of posterior bite plates, or an intrusive force such as a high head chin pull have been consid-ered, for the resolution of the anterior open bite, by creating an intrusion of posterior teeth. Some disad-vantages observed are discomfort functionally and esthetically of wearing a chin cup and functional discomfort of an occlusal bite plane. These systems also have the disadvantage of requiring a high degree of patient cooperation. The posterior segment intrusion technique has several advantages. It requires very little patient coop-eration. The technique has an excellent chance of working as long as the patient practices good oral hygiene and does not play with the mini screws. It does not interfere with the patient’s daily activities in social, esthetic or physical environments. The amount of intrusion force may be determined and adjusted as needed. The occlusal cant may be modified as needed as the forces may be adjusted, per the doctor’s criteria, independent of the patient’s cooperation. This case report presents the treatment rendered to an adolescent patient who presented with anterior open bite. She was treated with straight archwire sequence for initial alignment and leveling of the arches. The technique of using segmental arches allowed anterior extrusion and posterior intrusion combined with anterior elastics. The addition of intrusion forces of the posterior segments, based on bone anchorage with mini-screws placed on the buccal posterior segments, was introduced to allow a better control and result of the orthodontic treatment. Medical & Dental History SM, a teenage female, was seen in our office for orthodontic consultation at the age 12 years 11 months. The reason for the consultation was an ante-rior open bite. There was a history of thumb-sucking habit. After initial consultation, the patient and parent did not return until 16 months when the patient was 14 years 7 months of age. The severity of her anterior open bite was relatively unchanged with no evidence of spontaneous resolution, despite spite of the habit being discontinued for the past 16 months. A new medical history, dental examination and orthodontic evaluation were performed. Her medical history was unremarkable for allergies or medical problems. Her dental concerns included ante-rior open bite with a large diastema between the maxillary central incisors. Her dental exam, at the time of the initial orthodontic consult, revealed dental decay and gingivitis. There were no temporo-mandibular joint problems, but obvious skeletal and dental situations were in need of orthodontic and restorative corrections. The clinical orthodontic exam also revealed an occlusal cant imbalance and a noticeable facial asymmetry. Prior to the initiation of orthodontic treatment, her pertinent problems with gingivitis and dental decay were dealt with. “With this technique, it is possible to create a system that will allow the doctor to correct the anterior open bite without involving unnecessary extrusion of anterior teeth.” Clinical Analysis The oral exam revealed a Class I dental malocclusion with anterior overbite. The maxillary incisors were in protrusive angulation. The mandibular incisors had slight crowding. The molars in both arches were out of align-ment. Her open bite was 3 mm and her overjet was 7 mm. The midline was centered and even on both arches. The frontal image showed a tendency for a “gummy smile” due to excessive exposure of gingival soft tissue. (Fig 1) TMJ Examination The TMJ examination was within normal parame-ters. She related no prior history of headaches, joint dysfunction, pain or clenching and grinding. Upon clinical examination there was no popping, clicking or crepitus. The joint screening was within normal limits, with a vertical opening of 48 mm, a left deviation of 9 mm, and right deviation of 8 mm. www.orthodontics.com September/October 2011 25
Journal of the American Orthodontic Society September-October 2011: Page 25