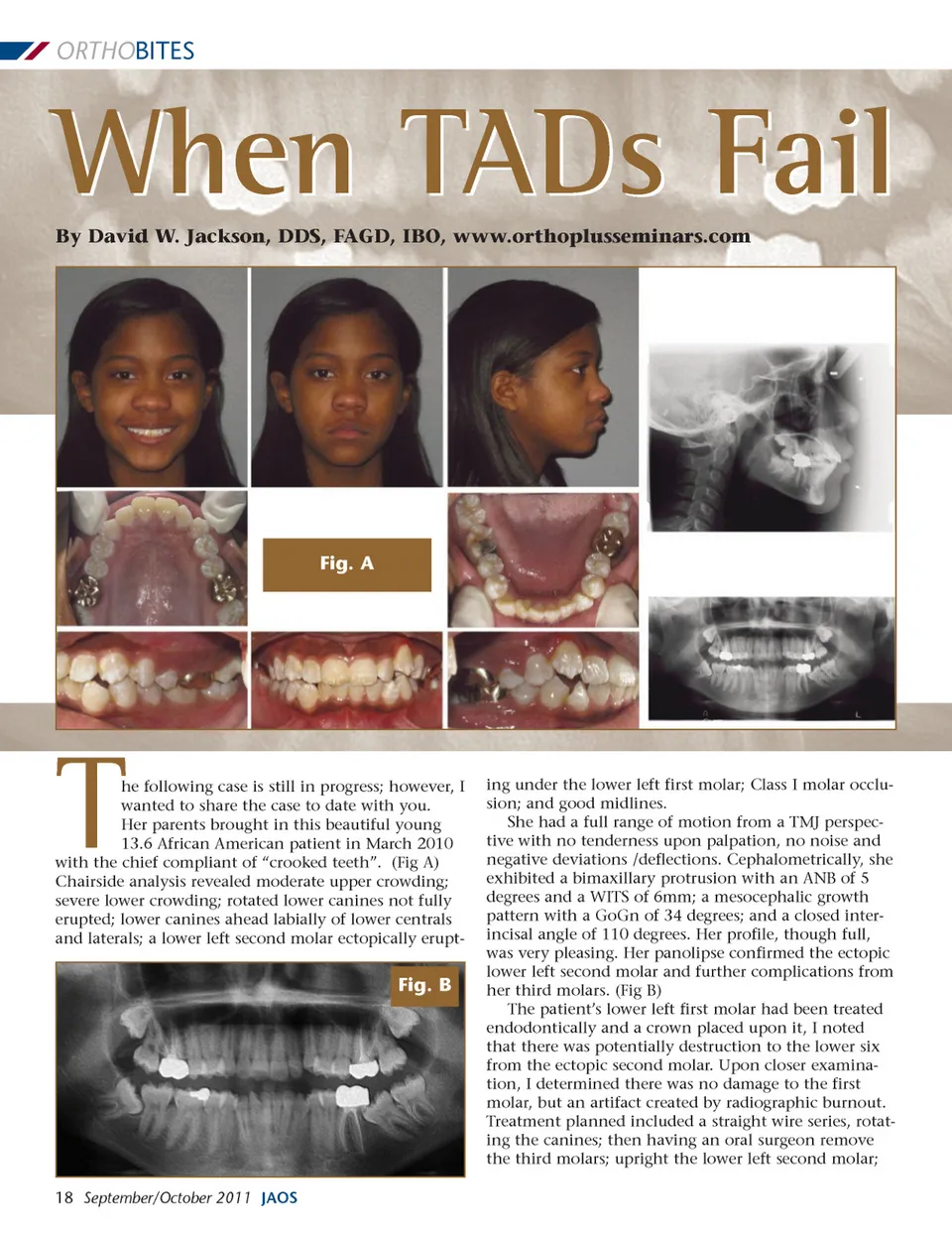
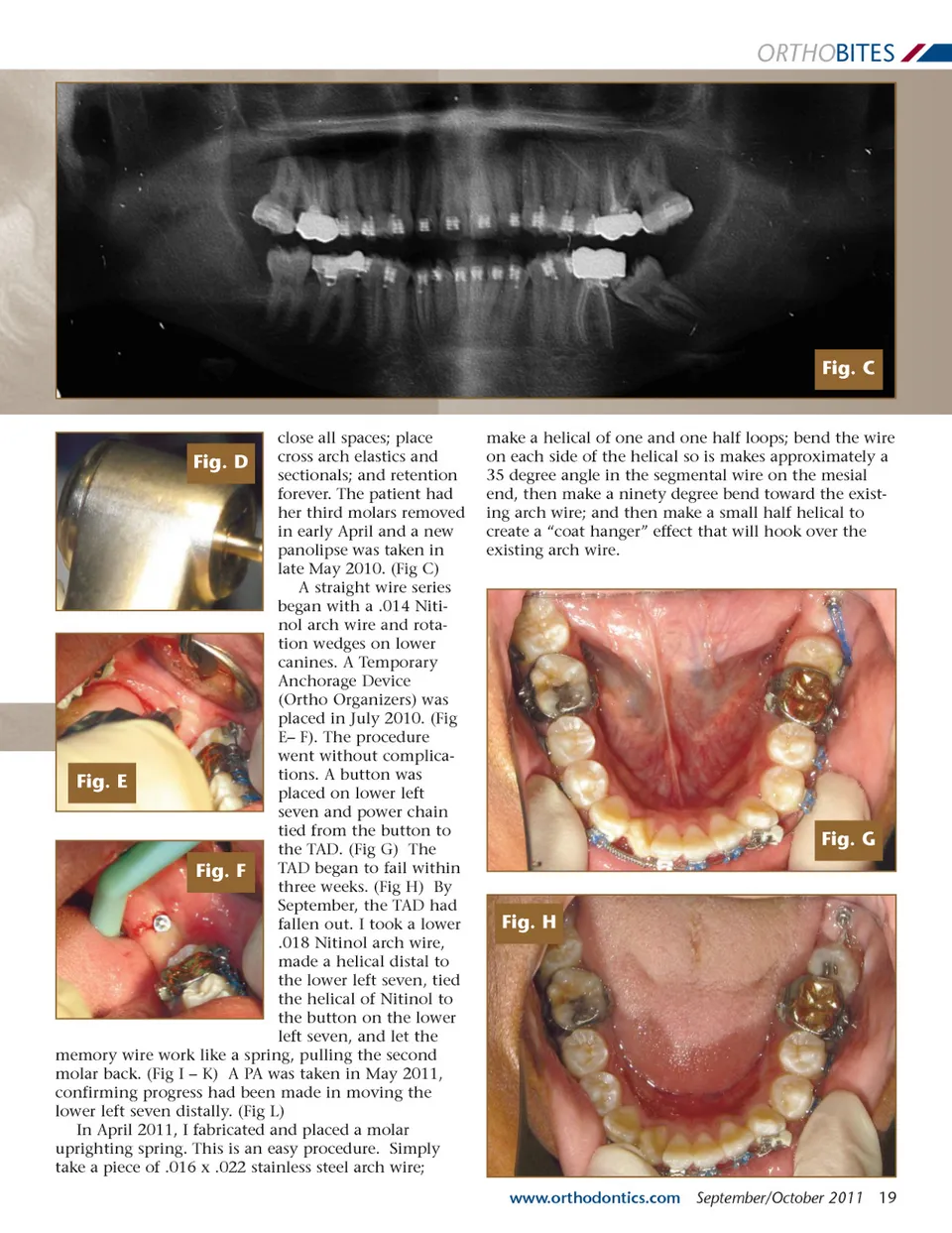
ORTHO BITES When TADs Fail By David W. Jackson, DDS, FAGD, IBO, www.orthoplusseminars.com Fig. A he following case is still in progress; however, I wanted to share the case to date with you. Her parents brought in this beautiful young 13.6 African American patient in March 2010 with the chief compliant of “crooked teeth”. (Fig A) Chairside analysis revealed moderate upper crowding; severe lower crowding; rotated lower canines not fully erupted; lower canines ahead labially of lower centrals and laterals; a lower left second molar ectopically erupt-T Fig. B ing under the lower left first molar; Class I molar occlu-sion; and good midlines. She had a full range of motion from a TMJ perspec-tive with no tenderness upon palpation, no noise and negative deviations /deflections. Cephalometrically, she exhibited a bimaxillary protrusion with an ANB of 5 degrees and a WITS of 6mm; a mesocephalic growth pattern with a GoGn of 34 degrees; and a closed inter-incisal angle of 110 degrees. Her profile, though full, was very pleasing. Her panolipse confirmed the ectopic lower left second molar and further complications from her third molars. (Fig B) The patient’s lower left first molar had been treated endodontically and a crown placed upon it, I noted that there was potentially destruction to the lower six from the ectopic second molar. Upon closer examina-tion, I determined there was no damage to the first molar, but an artifact created by radiographic burnout. Treatment planned included a straight wire series, rotat-ing the canines; then having an oral surgeon remove the third molars; upright the lower left second molar; 18 September/October 2011 JAOS
Journal of the American Orthodontic Society September-October 2011: Page 18