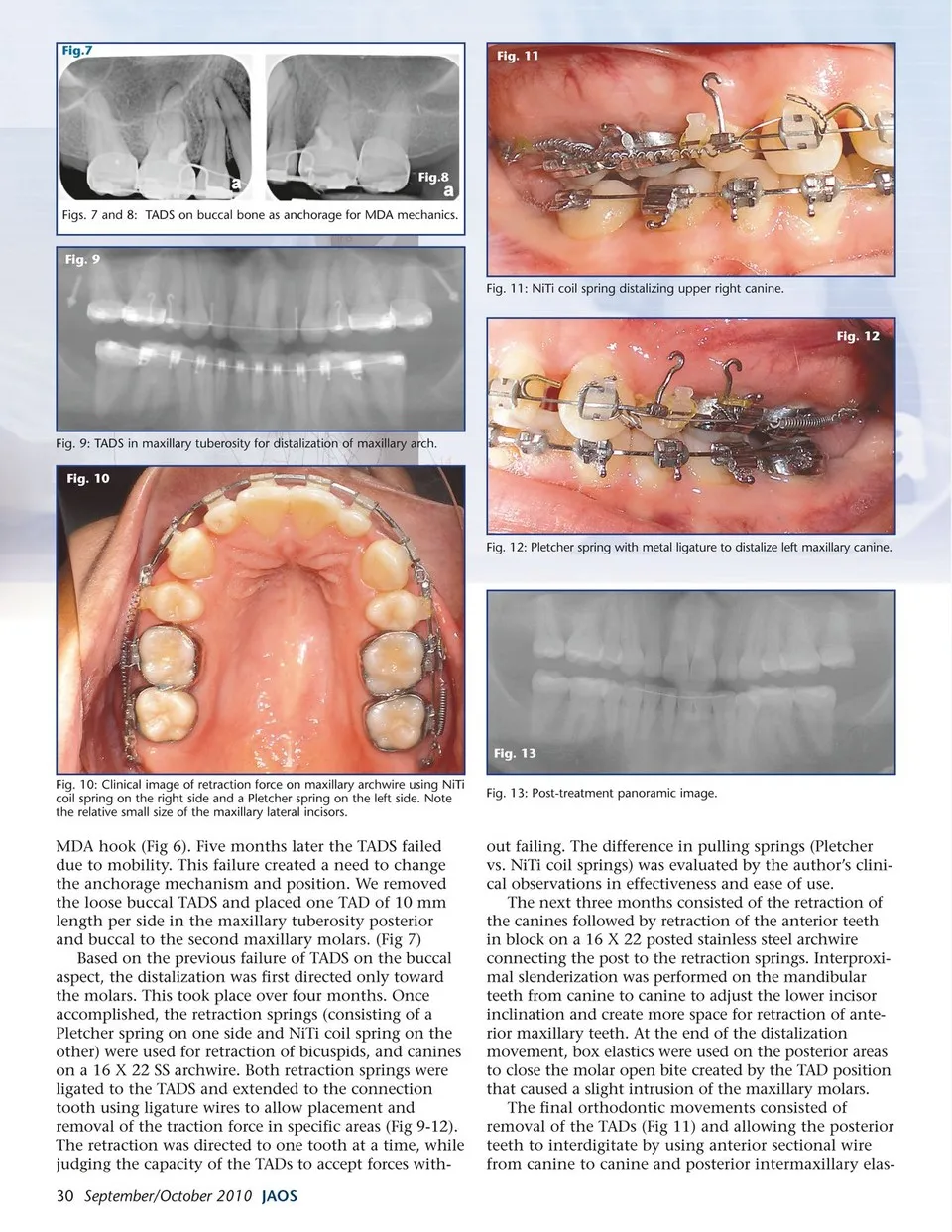
Fig.7 Fig. 11 Fig.8 Figs. 7 and 8: TADS on buccal bone as anchorage for MDA mechanics. Fig. 9 Fig. 11: NiTi coil spring distalizing upper right canine. Fig. 12 Fig. 9: TADS in maxillary tuberosity for distalization of maxillary arch. Fig. 10 Fig. 12: Pletcher spring with metal ligature to distalize left maxillary canine. Fig. 13 Fig. 10: Clinical image of retraction force on maxillary archwire using NiTi coil spring on the right side and a Pletcher spring on the left side. Note the relative small size of the maxillary lateral incisors. MDA hook (Fig 6). Five months later the TADS failed due to mobility. This failure created a need to change the anchorage mechanism and position. We removed the loose buccal TADS and placed one TAD of 10 mm length per side in the maxillary tuberosity posterior and buccal to the second maxillary molars. (Fig 7) Based on the previous failure of TADS on the buccal aspect, the distalization was first directed only toward the molars. This took place over four months. Once accomplished, the retraction springs (consisting of a Pletcher spring on one side and NiTi coil spring on the other) were used for retraction of bicuspids, and canines on a 16 X 22 SS archwire. Both retraction springs were ligated to the TADS and extended to the connection tooth using ligature wires to allow placement and removal of the traction force in specific areas (Fig 9-12). The retraction was directed to one tooth at a time, while judging the capacity of the TADs to accept forces with-30 September/October 2010 JAOS Fig. 13: Post-treatment panoramic image. out failing. The difference in pulling springs (Pletcher vs. NiTi coil springs) was evaluated by the author’s clini-cal observations in effectiveness and ease of use. The next three months consisted of the retraction of the canines followed by retraction of the anterior teeth in block on a 16 X 22 posted stainless steel archwire connecting the post to the retraction springs. Interproxi-mal slenderization was performed on the mandibular teeth from canine to canine to adjust the lower incisor inclination and create more space for retraction of ante-rior maxillary teeth. At the end of the distalization movement, box elastics were used on the posterior areas to close the molar open bite created by the TAD position that caused a slight intrusion of the maxillary molars. The final orthodontic movements consisted of removal of the TADs (Fig 11) and allowing the posterior teeth to interdigitate by using anterior sectional wire from canine to canine and posterior intermaxillary elas-
Journal of the American Orthodontic Society September-October 2010: Page 30