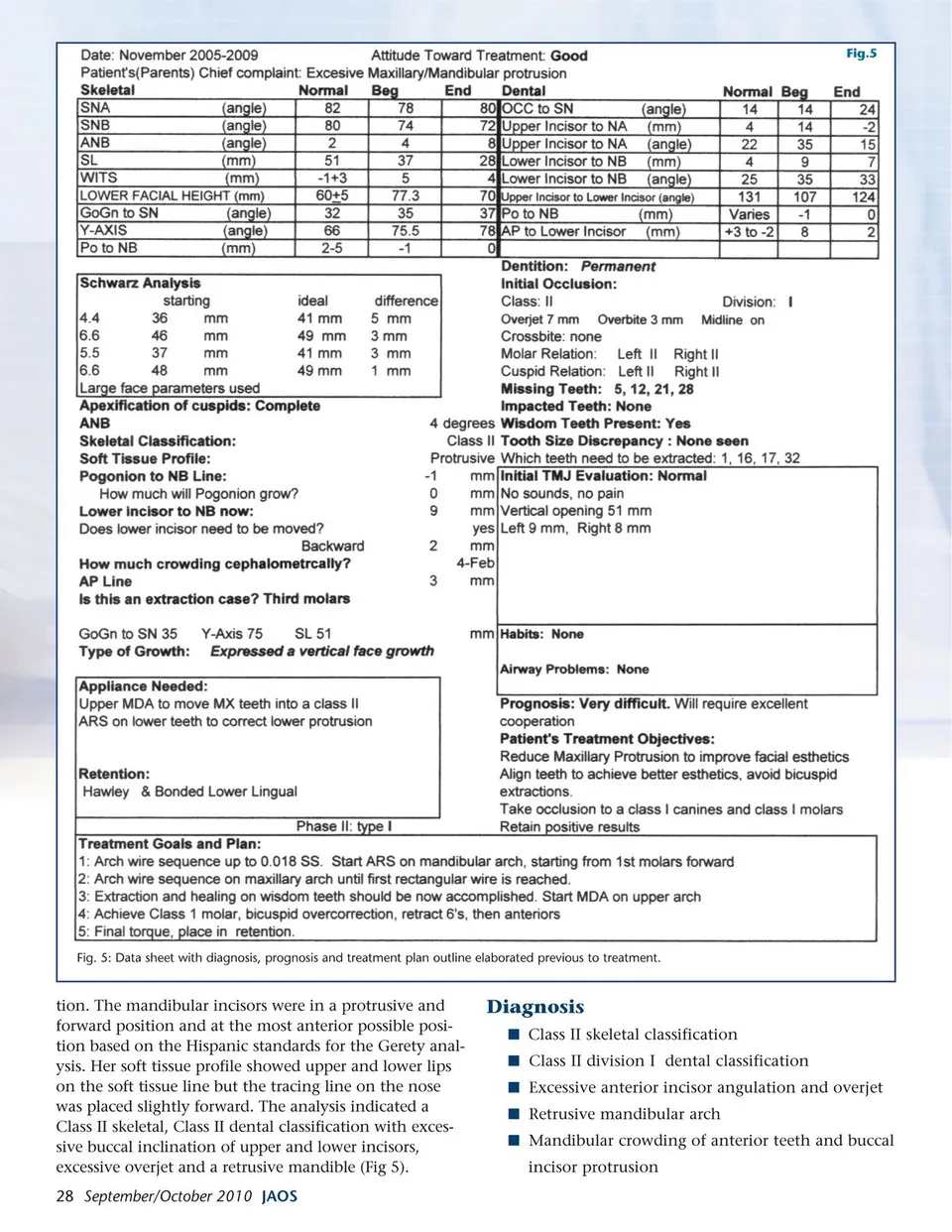
Fig.6 Fig. 6: MDA distalizing appliance combined with TADS as anchorage points. Treatment Objectives Improve facial and dental esthetics Align and level teeth in their arches Correct rotations and crowding of anterior teeth Reduce excessive maxillary incisor protrusion and excessive overjet Reduce excessive mandibular incisor labial protrusion Reduce lip strain caused by the positioning of the anterior teeth Achieve a bilateral Class I molar and Class I canine occlusion Retain positive results over time Treatment Plan Straight Wire Appliances with routine archwire sequence Level, align and rotate the upper and lower arches Reduce lower incisor crowding and protrusion with dental interproximal slenderization3 Use an MDA to take the upper arch into a Class I relationship with the mandibular arch Coordinate the arches into Class I molar and Class I canine occlusion Obtain a positive overbite and overjet. Obtain solid posterior occlusal stability with a combina-tion maxillary Hawley retainer and bonded lower lingual retainer to keep teeth in a Class I occlusion Long term retention and recall visits protocol Estimated Treatment Time 24-36 months Case Summary and Analysis HG was seen in our office for an orthodontic consul-tation at 28 years of age. A clinical exam was performed and the need for records was explained and scheduled. Orthodontic records were taken and analyzed. A consultation was obtained from Dr. Gerety involving diagnosis and treatment planning. The patient’s diag-nosis was completed and a treatment plan was prepared for presentation. For four months the patient was treated with arch wire sequence (AWS) preparing the arches for the protocol of MDA distalization (Multi-Distalizing Arch) as taught by Dr. Gerety in his course “Straight Wire Concepts: Diagnosis and Technique”2 and by Dr. Jackson in his course “The Next Step”4 At the end of the third month of treatment, it was possible to bracket and move tooth # 25 lingually, into the arch perimeter, where it had previously been blocked out. At this time, in preparation for the maxillary molar distalization to be done in the near future, the four third molars were removed under local anesthesia and conscious sedation, with no complications. In the fifth month of treatment an MDA size # 5 was installed with the standard instructions of 3 medium elastics of ¼ (3 X 4.5 oz = 13.5 oz)1 . The lower arch was treated with interproxi-mal slenderization and single tooth retraction, starting from the mandibular first molars and moving in a mesial direction, closing the spaces created with power chain elastics.6 , for one week and then two elastics of ¼ (9 oz) until the next activation. Our objective was the distalization of the maxillary molars into a class I relationship. After four months of distalization, a MDA # 6 was placed to continue retrac-tion. Spacing occurred between the maxillary teeth caused by the patient’s improper use of the anchorage elastics. The need to use anchorage elastics to prevent negative secondary movements was discussed with HG and the attempt to complete distalization continued for six more months. The MDA was removed after it was observed that the patient was not wearing the required elastics to prevent buccal movement of the anterior maxillary teeth. Diastemas were created on all areas mesial to the first molars. The patient’s reason for not wearing the required elastics was that intense pain in the temporo-mandibular joints resulted when using the elastics for intermaxillary anchorage. It was obvious there was a problem with this type of mechanical approach to distalization. The patient was extremely cooperative, in all other aspects of the therapy, and had extensive knowledge of the treatment and its objec-tives, but her pain was stronger than the desire to improve the dental malocclusion. Closing the diastemas that formed by the MDA, due to improper anchorage, took three months of treat-ment. The patient continued in a Class II molar and Class II canine relationship. The MDA technique was revisited in an attempt to continue distalization of the molars into a Class I relationship. The strategy devised was to use temporary anchorage devices (TADs) in the form of mini screw implants (MSI) as anchorage to prevent flaring of the incisors. Two TADS of 6 mm length were placed after one month on the maxillary arch along the buccal area between first molars and second bicuspids to use as anchorage for the MDA appliance (Fig 5 and 6). The patient was asked to use three elastics per side (13.5 oz.) from the TAD to the www.orthodontics.com September/October 2010 29
Journal of the American Orthodontic Society September-October 2010: Page 29