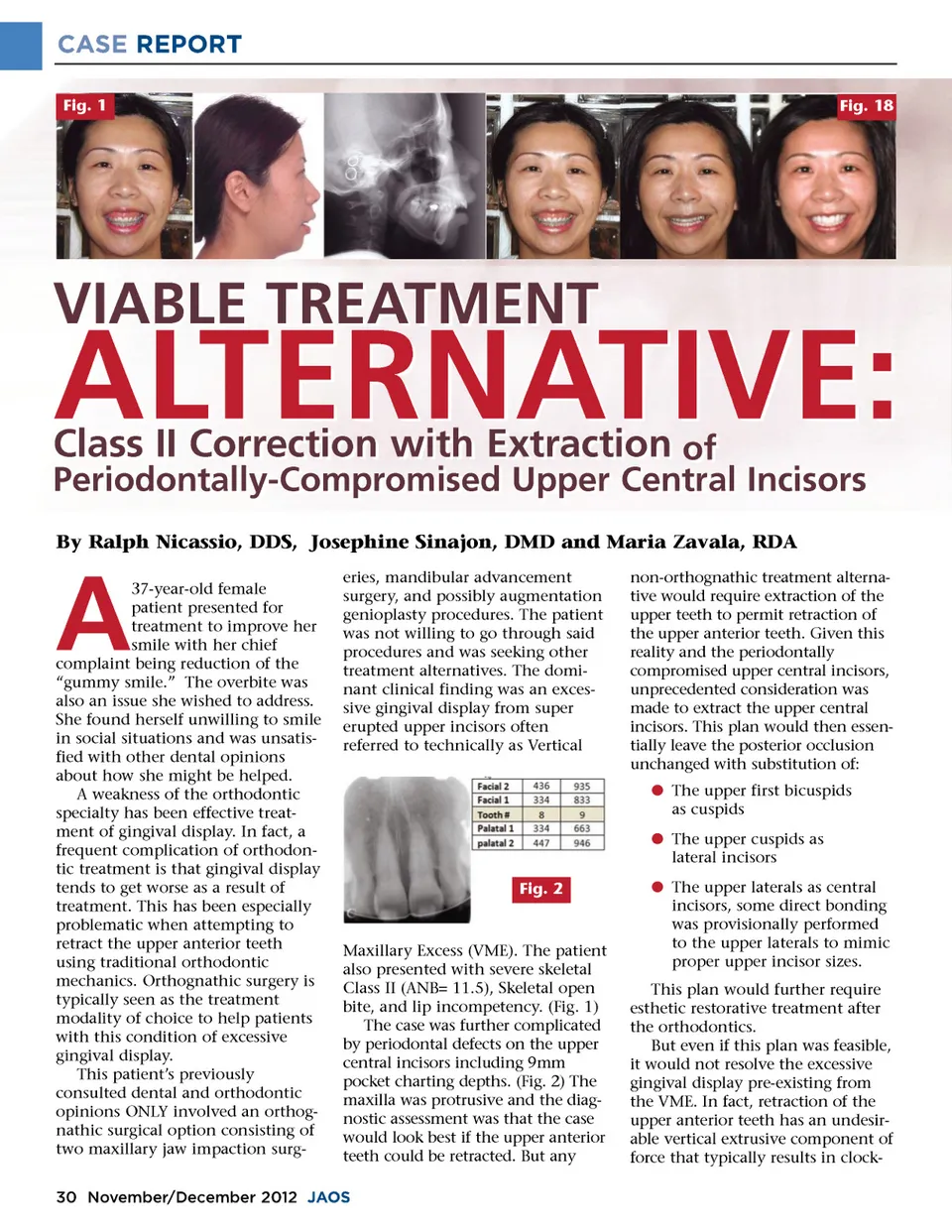
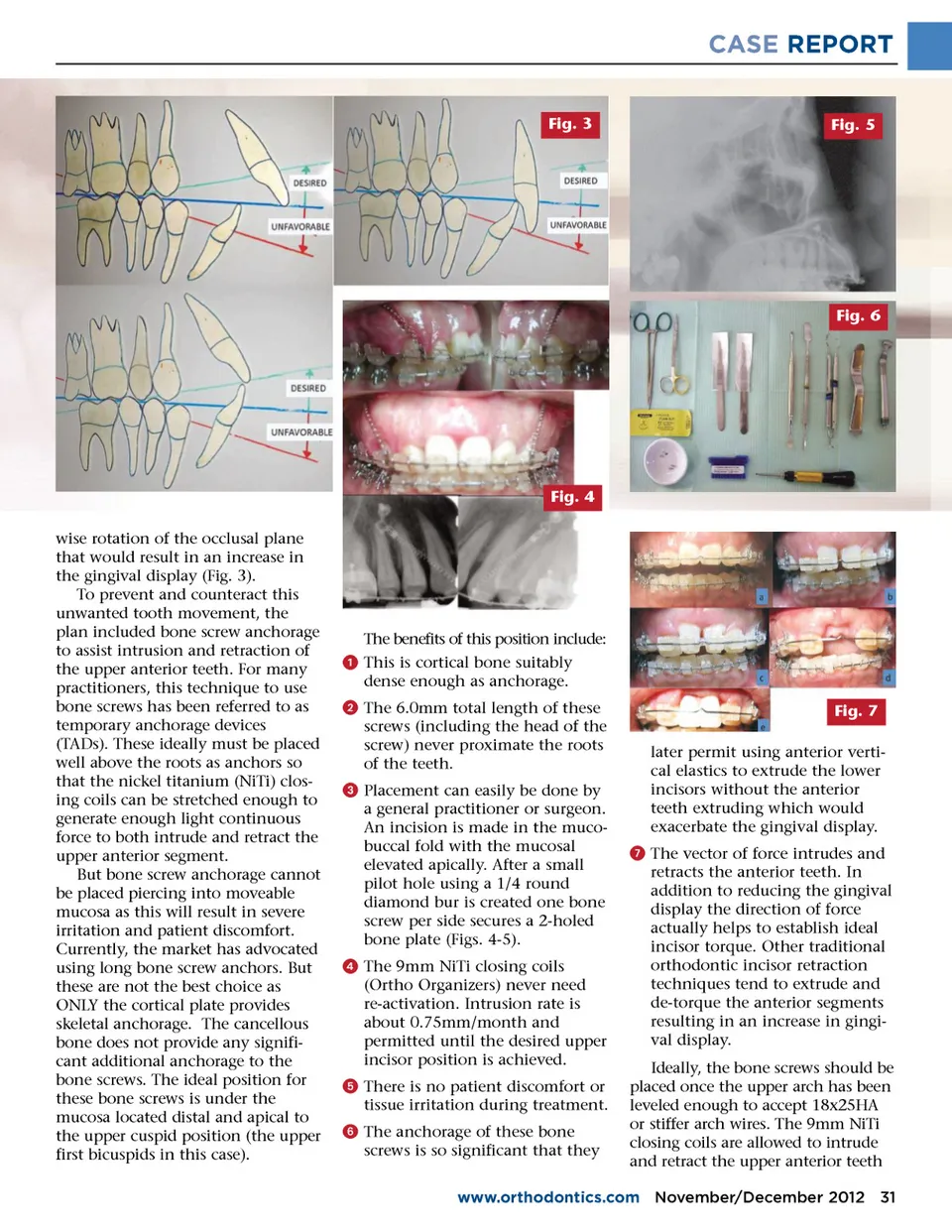
CASE REPORT Fig. 1 Fig. 18 VIABLE TREATMENT ALTERNATIVE: Periodontally-Compromised Upper Central Incisors By Ralph Nicassio, DDS, Josephine Sinajon, DMD and Maria Zavala, RDA Class II Correction with Extraction of A 37-year-old female patient presented for treatment to improve her smile with her chief complaint being reduction of the “gummy smile.” The overbite was also an issue she wished to address. She found herself unwilling to smile in social situations and was unsatis-fied with other dental opinions about how she might be helped. A weakness of the orthodontic specialty has been effective treat-ment of gingival display. In fact, a frequent complication of orthodon-tic treatment is that gingival display tends to get worse as a result of treatment. This has been especially problematic when attempting to retract the upper anterior teeth using traditional orthodontic mechanics. Orthognathic surgery is typically seen as the treatment modality of choice to help patients with this condition of excessive gingival display. This patient’s previously consulted dental and orthodontic opinions ONLY involved an orthog-nathic surgical option consisting of two maxillary jaw impaction surg-eries, mandibular advancement surgery, and possibly augmentation genioplasty procedures. The patient was not willing to go through said procedures and was seeking other treatment alternatives. The domi-nant clinical finding was an exces-sive gingival display from super erupted upper incisors often referred to technically as Vertical non-orthognathic treatment alterna-tive would require extraction of the upper teeth to permit retraction of the upper anterior teeth. Given this reality and the periodontally compromised upper central incisors, unprecedented consideration was made to extract the upper central incisors. This plan would then essen-tially leave the posterior occlusion unchanged with substitution of: b The upper first bicuspids as cuspids b The upper cuspids as lateral incisors Fig. 2 Maxillary Excess (VME). The patient also presented with severe skeletal Class II (ANB= 11.5), Skeletal open bite, and lip incompetency. (Fig. 1) The case was further complicated by periodontal defects on the upper central incisors including 9mm pocket charting depths. (Fig. 2) The maxilla was protrusive and the diag-nostic assessment was that the case would look best if the upper anterior teeth could be retracted. But any b The upper laterals as central incisors, some direct bonding was provisionally performed to the upper laterals to mimic proper upper incisor sizes. This plan would further require esthetic restorative treatment after the orthodontics. But even if this plan was feasible, it would not resolve the excessive gingival display pre-existing from the VME. In fact, retraction of the upper anterior teeth has an undesir-able vertical extrusive component of force that typically results in clock-30 November/December 2012 JAOS
Journal of the American Orthodontic Society November-December 2012: Page 30