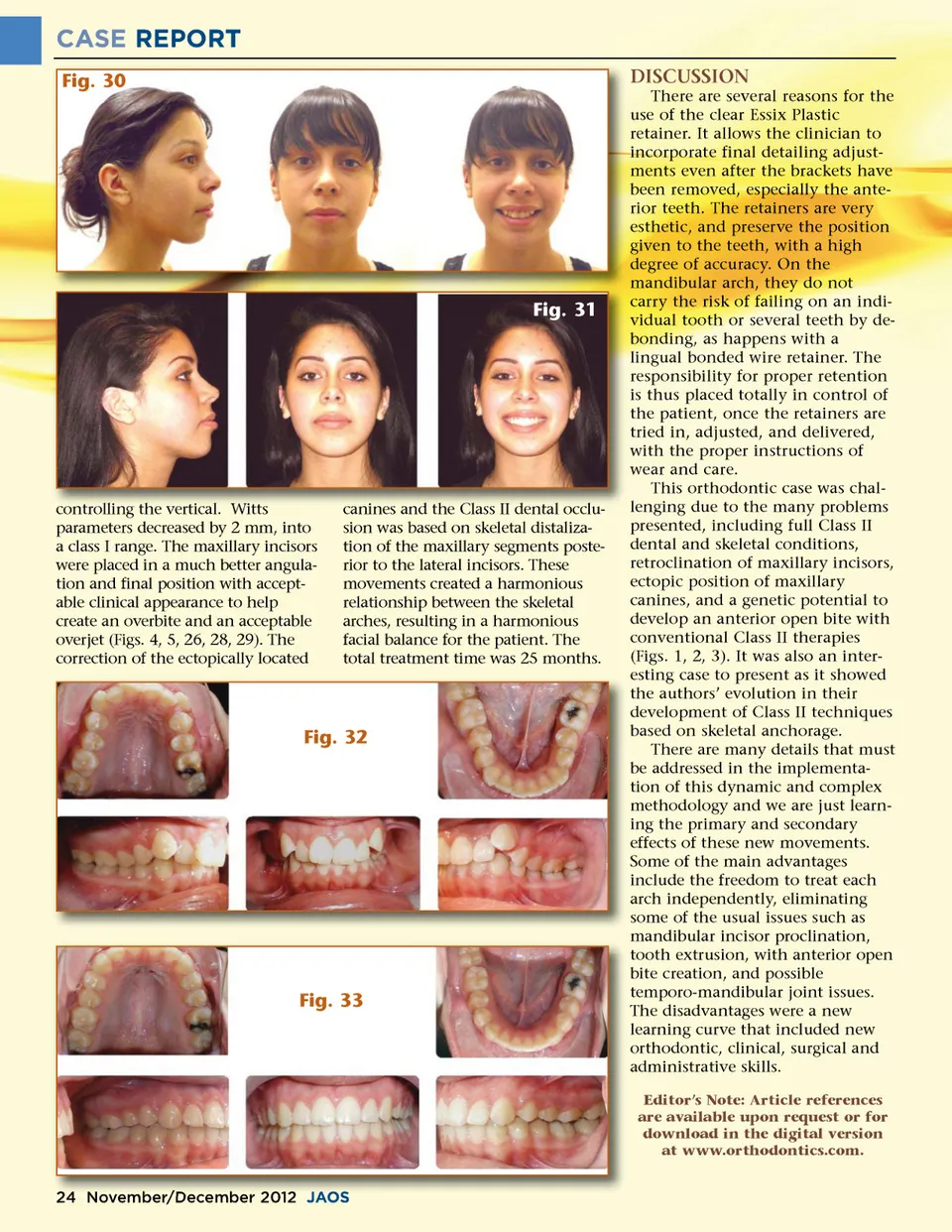
CASE REPORT Fig. 30 DISCUSSION There are several reasons for the use of the clear Essix Plastic retainer. It allows the clinician to incorporate final detailing adjust-ments even after the brackets have been removed, especially the ante-rior teeth. The retainers are very esthetic, and preserve the position given to the teeth, with a high degree of accuracy. On the mandibular arch, they do not carry the risk of failing on an indi-vidual tooth or several teeth by de-bonding, as happens with a lingual bonded wire retainer. The responsibility for proper retention is thus placed totally in control of the patient, once the retainers are tried in, adjusted, and delivered, with the proper instructions of wear and care. This orthodontic case was chal-lenging due to the many problems presented, including full Class II dental and skeletal conditions, retroclination of maxillary incisors, ectopic position of maxillary canines, and a genetic potential to develop an anterior open bite with conventional Class II therapies (Figs. 1, 2, 3). It was also an inter-esting case to present as it showed the authors’ evolution in their development of Class II techniques based on skeletal anchorage. There are many details that must be addressed in the implementa-tion of this dynamic and complex methodology and we are just learn-ing the primary and secondary effects of these new movements. Some of the main advantages include the freedom to treat each arch independently, eliminating some of the usual issues such as mandibular incisor proclination, tooth extrusion, with anterior open bite creation, and possible temporo-mandibular joint issues. The disadvantages were a new learning curve that included new orthodontic, clinical, surgical and administrative skills. Editor’s Note: Article references are available upon request or for download in the digital version at www.orthodontics.com. Fig. 31 controlling the vertical. vertical Witts W tts Wi parameters decreased by 2 mm, into a class I range. The maxillary incisors were placed in a much better angula-tion and final position with accept-able clinical appearance to help create an overbite and an acceptable overjet (Figs. 4, 5, 26, 28, 29). The correction of the ectopically located canines and the Class II dental occlu-occlu sion was based on skeletal distaliza-tion of the maxillary segments poste-rior to the lateral incisors. These movements created a harmonious relationship between the skeletal arches, resulting in a harmonious facial balance for the patient. The total treatment time was 25 months. Fig. 32 Fig. 33 24 November/December November/ r December 2012 J JAOS AOS
Journal of the American Orthodontic Society November-December 2012: Page 24