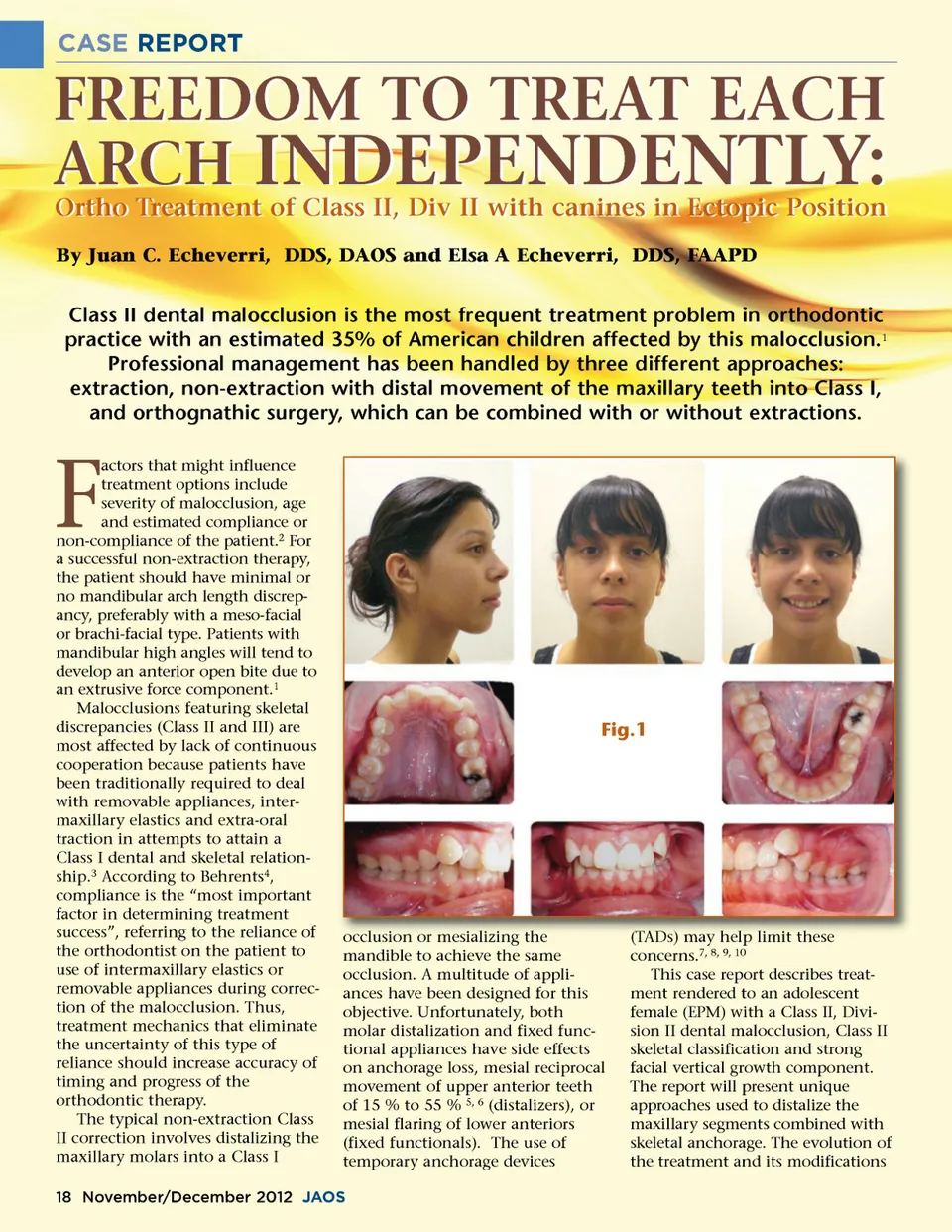
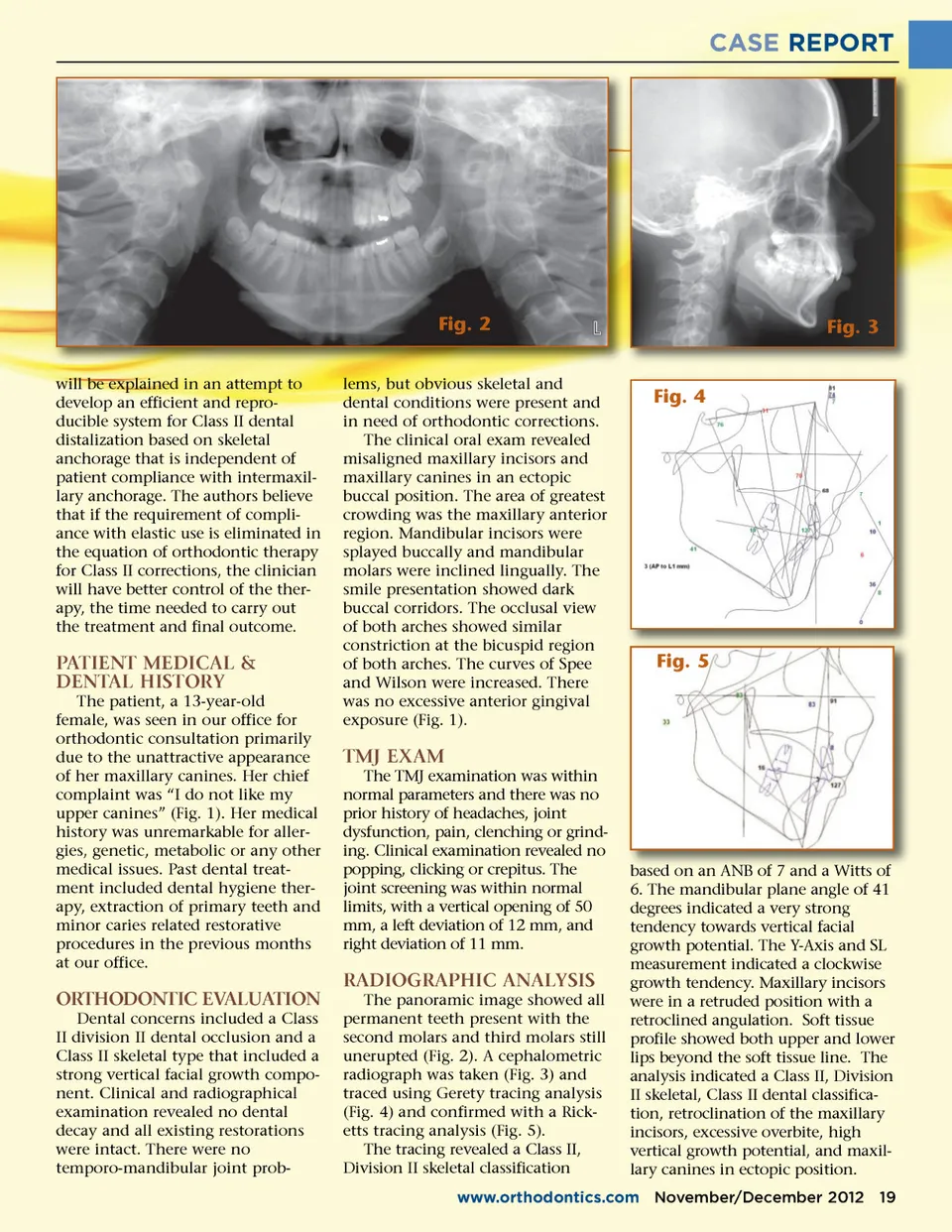
CASE REPORT Fig. 2 will be explained in an attempt to develop an efficient and repro-ducible system for Class II dental distalization based on skeletal anchorage that is independent of patient compliance with intermaxil-lary anchorage. The authors believe that if the requirement of compli-ance with elastic use is eliminated in the equation of orthodontic therapy for Class II corrections, the clinician will have better control of the ther-apy, the time needed to carry out the treatment and final outcome. lems, but obvious skeletal and dental conditions were present and in need of orthodontic corrections. The clinical oral exam revealed misaligned maxillary incisors and maxillary canines in an ectopic buccal position. The area of greatest crowding was the maxillary anterior region. Mandibular incisors were splayed buccally and mandibular molars were inclined lingually. The smile presentation showed dark buccal corridors. The occlusal view of both arches showed similar constriction at the bicuspid region of both arches. The curves of Spee and Wilson were increased. There was no excessive anterior gingival exposure (Fig. 1). Fig. 3 Fig. 4 PATIENT MEDICAL & DENTAL HISTORY The patient, a 13-year-old female, was seen in our office for orthodontic consultation primarily due to the unattractive appearance of her maxillary canines. Her chief complaint was “I do not like my upper canines” (Fig. 1). Her medical history was unremarkable for aller-gies, genetic, metabolic or any other medical issues. Past dental treat-ment included dental hygiene ther-apy, extraction of primary teeth and minor caries related restorative procedures in the previous months at our office. Fig. 5 TMJ EXAM The TMJ examination was within normal parameters and there was no prior history of headaches, joint dysfunction, pain, clenching or grind-ing. Clinical examination revealed no popping, clicking or crepitus. The joint screening was within normal limits, with a vertical opening of 50 mm, a left deviation of 12 mm, and right deviation of 11 mm. RADIOGRAPHIC ANALYSIS ORTHODONTIC EVALUATION Dental concerns included a Class II division II dental occlusion and a Class II skeletal type that included a strong vertical facial growth compo-nent. Clinical and radiographical examination revealed no dental decay and all existing restorations were intact. There were no temporo-mandibular joint prob-The panoramic image showed all permanent teeth present with the second molars and third molars still unerupted (Fig. 2). A cephalometric radiograph was taken (Fig. 3) and traced using Gerety tracing analysis (Fig. 4) and confirmed with a Rick-etts tracing analysis (Fig. 5). The tracing revealed a Class II, Division II skeletal classification based on an ANB of 7 and a Witts of 6. The mandibular plane angle of 41 degrees indicated a very strong tendency towards vertical facial growth potential. The Y-Axis and SL measurement indicated a clockwise growth tendency. Maxillary incisors were in a retruded position with a retroclined angulation. Soft tissue profile showed both upper and lower lips beyond the soft tissue line. The analysis indicated a Class II, Division II skeletal, Class II dental classifica-tion, retroclination of the maxillary incisors, excessive overbite, high vertical growth potential, and maxil-lary canines in ectopic position. www.orthodontics.com November/December 2012 19
Journal of the American Orthodontic Society November-December 2012: Page 19