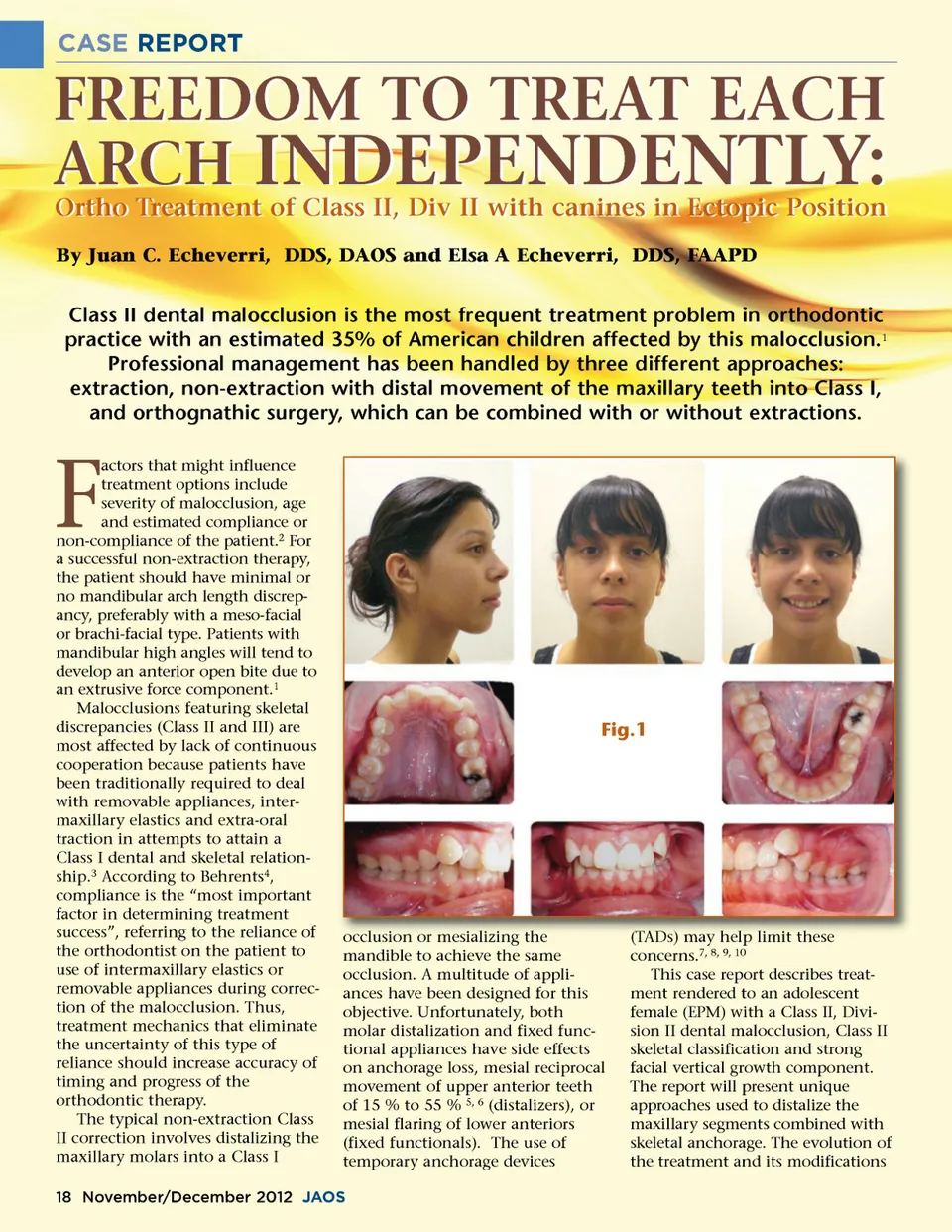
CASE REPORT FREEDOM TO TREAT EACH ARCH INDEPENDENTLY: Ortho Treatment of Class II, Div II with canines in Ectopic Position By Juan C. Echeverri, DDS, DAOS and Elsa A Echeverri, DDS, FAAPD Class II dental malocclusion is the most frequent treatment problem in orthodontic practice with an estimated 35% of American children affected by this malocclusion. 1 Professional management has been handled by three different approaches: extraction, non-extraction with distal movement of the maxillary teeth into Class I, and orthognathic surgery, which can be combined with or without extractions. F actors that might influence treatment options include severity of malocclusion, age and estimated compliance or non-compliance of the patient. 2 For a successful non-extraction therapy, the patient should have minimal or no mandibular arch length discrep-ancy, preferably with a meso-facial or brachi-facial type. Patients with mandibular high angles will tend to develop an anterior open bite due to an extrusive force component. 1 Malocclusions featuring skeletal discrepancies (Class II and III) are most affected by lack of continuous cooperation because patients have been traditionally required to deal with removable appliances, inter-maxillary elastics and extra-oral traction in attempts to attain a Class I dental and skeletal relation-ship. 3 According to Behrents 4 , compliance is the “most important factor in determining treatment success”, referring to the reliance of the orthodontist on the patient to use of intermaxillary elastics or removable appliances during correc-tion of the malocclusion. Thus, treatment mechanics that eliminate the uncertainty of this type of reliance should increase accuracy of timing and progress of the orthodontic therapy. The typical non-extraction Class II correction involves distalizing the maxillary molars into a Class I Fig.1 occlusion or mesializing the mandible to achieve the same occlusion. A multitude of appli-ances have been designed for this objective. Unfortunately, both molar distalization and fixed func-tional appliances have side effects on anchorage loss, mesial reciprocal movement of upper anterior teeth of 15 % to 55 % 5, 6 (distalizers), or mesial flaring of lower anteriors (fixed functionals). The use of temporary anchorage devices (TADs) (TA T Ds) may help limit these concerns. 7, 8, 9, 10 This case report describes treat-ment rendered to an adolescent female (EPM) with a Class II, Divi-sion II dental malocclusion, Class II skeletal classification and strong facial vertical growth component. The report will present unique approaches used to distalize the maxillary segments combined with skeletal anchorage. The evolution of the treatment and its modifications 18 November/December 2012 JAOS
Journal of the American Orthodontic Society November-December 2012: Page 18