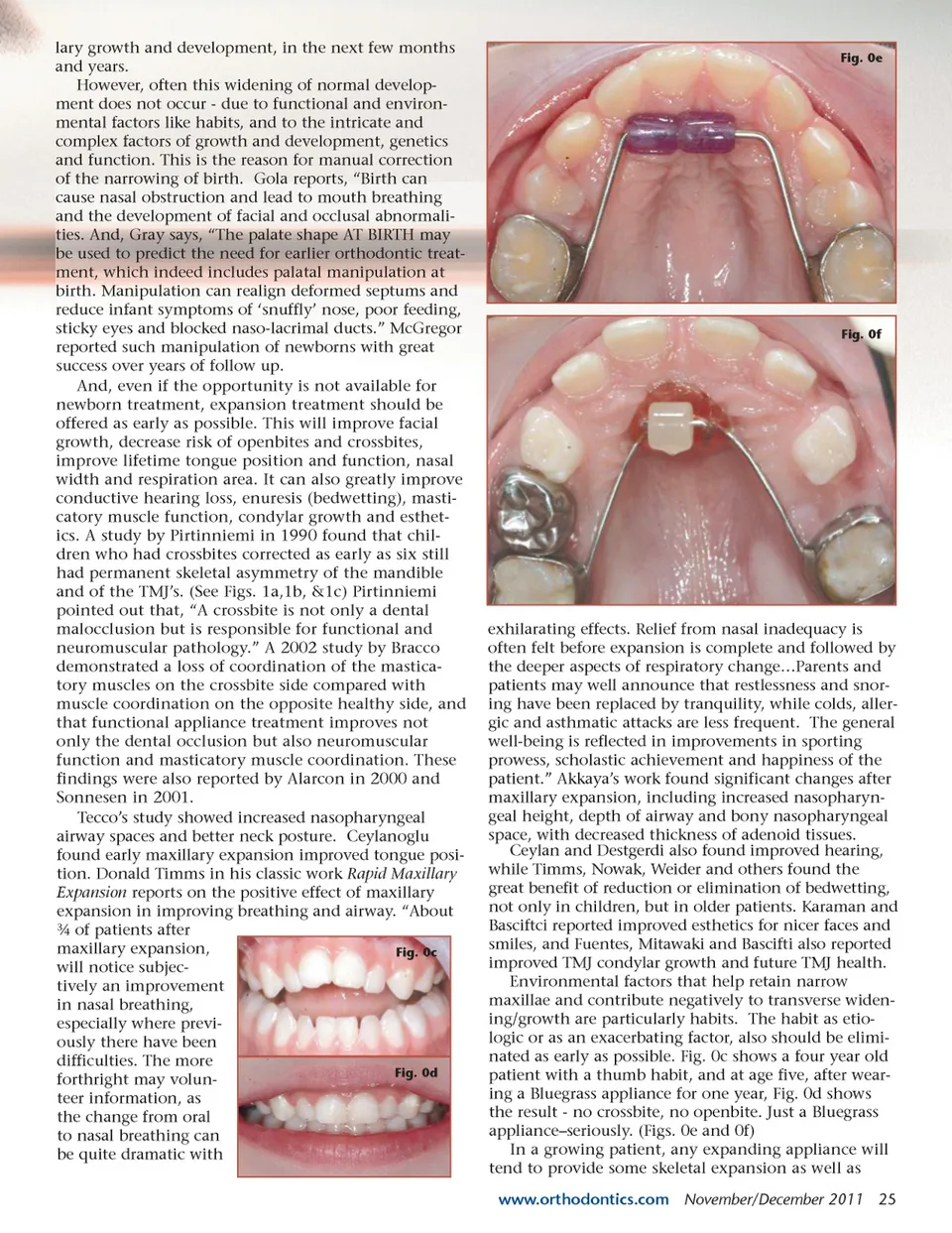
lary growth and development, in the next few months and years. However, often this widening of normal develop-ment does not occur -due to functional and environ-mental factors like habits, and to the intricate and complex factors of growth and development, genetics and function. This is the reason for manual correction of the narrowing of birth. Gola reports, “Birth can cause nasal obstruction and lead to mouth breathing and the development of facial and occlusal abnormali-ties. And, Gray says, “The palate shape AT BIRTH may be used to predict the need for earlier orthodontic treat-ment, which indeed includes palatal manipulation at birth. Manipulation can realign deformed septums and reduce infant symptoms of ‘snuffly’ nose, poor feeding, sticky eyes and blocked naso-lacrimal ducts.” McGregor reported such manipulation of newborns with great success over years of follow up. And, even if the opportunity is not available for newborn treatment, expansion treatment should be offered as early as possible. This will improve facial growth, decrease risk of openbites and crossbites, improve lifetime tongue position and function, nasal width and respiration area. It can also greatly improve conductive hearing loss, enuresis (bedwetting), masti-catory muscle function, condylar growth and esthet-ics. A study by Pirtinniemi in 1990 found that chil-dren who had crossbites corrected as early as six still had permanent skeletal asymmetry of the mandible and of the TMJ’s. (See Figs. 1a,1b, &1c) Pirtinniemi pointed out that, “A crossbite is not only a dental malocclusion but is responsible for functional and neuromuscular pathology.” A 2002 study by Bracco demonstrated a loss of coordination of the mastica-tory muscles on the crossbite side compared with muscle coordination on the opposite healthy side, and that functional appliance treatment improves not only the dental occlusion but also neuromuscular function and masticatory muscle coordination. These findings were also reported by Alarcon in 2000 and Sonnesen in 2001. Tecco’s study showed increased nasopharyngeal airway spaces and better neck posture. Ceylanoglu found early maxillary expansion improved tongue posi-tion. Donald Timms in his classic work Rapid Maxillary Expansion reports on the positive effect of maxillary expansion in improving breathing and airway. “About ¾ of patients after maxillary expansion, Fig. 0c will notice subjec-tively an improvement in nasal breathing, especially where previ-ously there have been difficulties. The more Fig. 0d forthright may volun-teer information, as the change from oral to nasal breathing can be quite dramatic with Fig. 0e Fig. 0f exhilarating effects. Relief from nasal inadequacy is often felt before expansion is complete and followed by the deeper aspects of respiratory change…Parents and patients may well announce that restlessness and snor-ing have been replaced by tranquility, while colds, aller-gic and asthmatic attacks are less frequent. The general well-being is reflected in improvements in sporting prowess, scholastic achievement and happiness of the patient.” Akkaya’s work found significant changes after maxillary expansion, including increased nasopharyn-geal height, depth of airway and bony nasopharyngeal space, with decreased thickness of adenoid tissues. Ceylan and Destgerdi also found improved hearing, while Timms, Nowak, Weider and others found the great benefit of reduction or elimination of bedwetting, not only in children, but in older patients. Karaman and Basciftci reported improved esthetics for nicer faces and smiles, and Fuentes, Mitawaki and Bascifti also reported improved TMJ condylar growth and future TMJ health. Environmental factors that help retain narrow maxillae and contribute negatively to transverse widen-ing/growth are particularly habits. The habit as etio-logic or as an exacerbating factor, also should be elimi-nated as early as possible. Fig. 0c shows a four year old patient with a thumb habit, and at age five, after wear-ing a Bluegrass appliance for one year, Fig. 0d shows the result -no crossbite, no openbite. Just a Bluegrass appliance–seriously. (Figs. 0e and 0f) In a growing patient, any expanding appliance will tend to provide some skeletal expansion as well as www.orthodontics.com November/December 2011 25
Journal of the American Orthodontic Society November-December 2011: Page 25