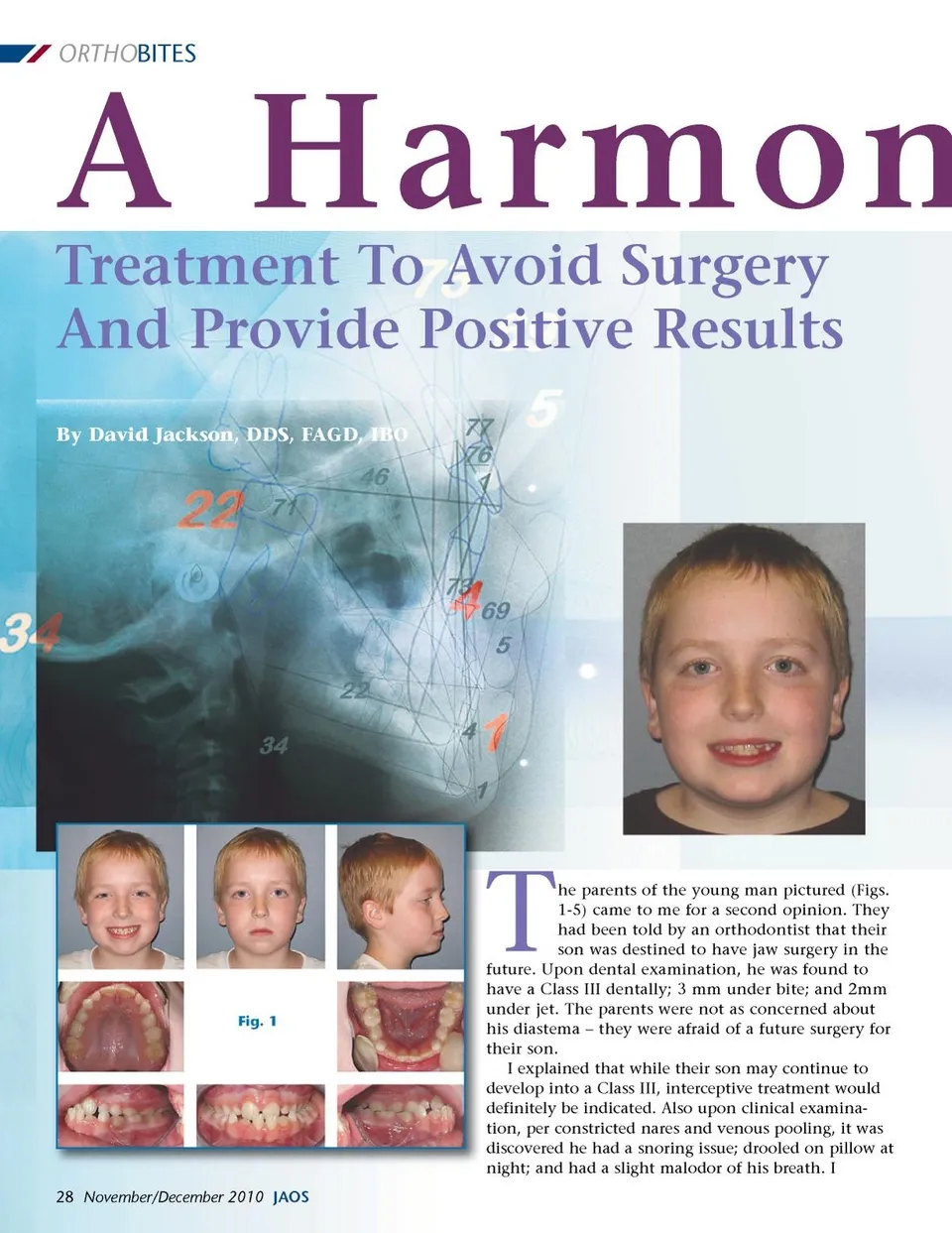
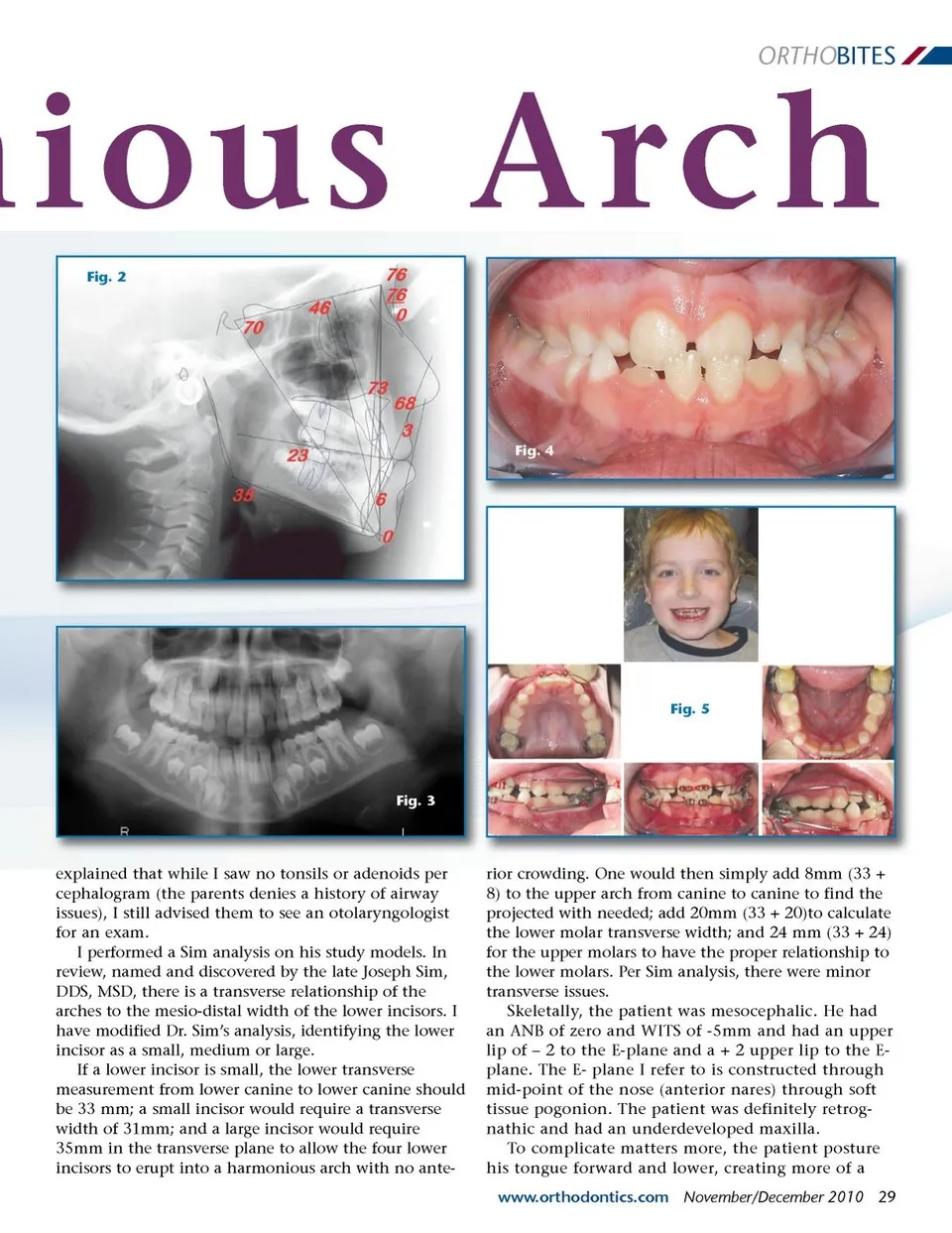
ORTHO BITES nious Arch Fig. 2 Fig. 4 Fig. 5 Fig. 3 explained that while I saw no tonsils or adenoids per cephalogram (the parents denies a history of airway issues), I still advised them to see an otolaryngologist for an exam. I performed a Sim analysis on his study models. In review, named and discovered by the late Joseph Sim, DDS, MSD, there is a transverse relationship of the arches to the mesio-distal width of the lower incisors. I have modified Dr. Sim’s analysis, identifying the lower incisor as a small, medium or large. If a lower incisor is small, the lower transverse measurement from lower canine to lower canine should be 33 mm; a small incisor would require a transverse width of 31mm; and a large incisor would require 35mm in the transverse plane to allow the four lower incisors to erupt into a harmonious arch with no ante-rior crowding. One would then simply add 8mm (33 + 8) to the upper arch from canine to canine to find the projected with needed; add 20mm (33 + 20)to calculate the lower molar transverse width; and 24 mm (33 + 24) for the upper molars to have the proper relationship to the lower molars. Per Sim analysis, there were minor transverse issues. Skeletally, the patient was mesocephalic. He had an ANB of zero and WITS of -5mm and had an upper lip of – 2 to the E-plane and a + 2 upper lip to the E-plane. The E-plane I refer to is constructed through mid-point of the nose (anterior nares) through soft tissue pogonion. The patient was definitely retrog-nathic and had an underdeveloped maxilla. To complicate matters more, the patient posture his tongue forward and lower, creating more of a www.orthodontics.com November/December 2010 29
Journal of the American Orthodontic Society November-December 2010: Page 29