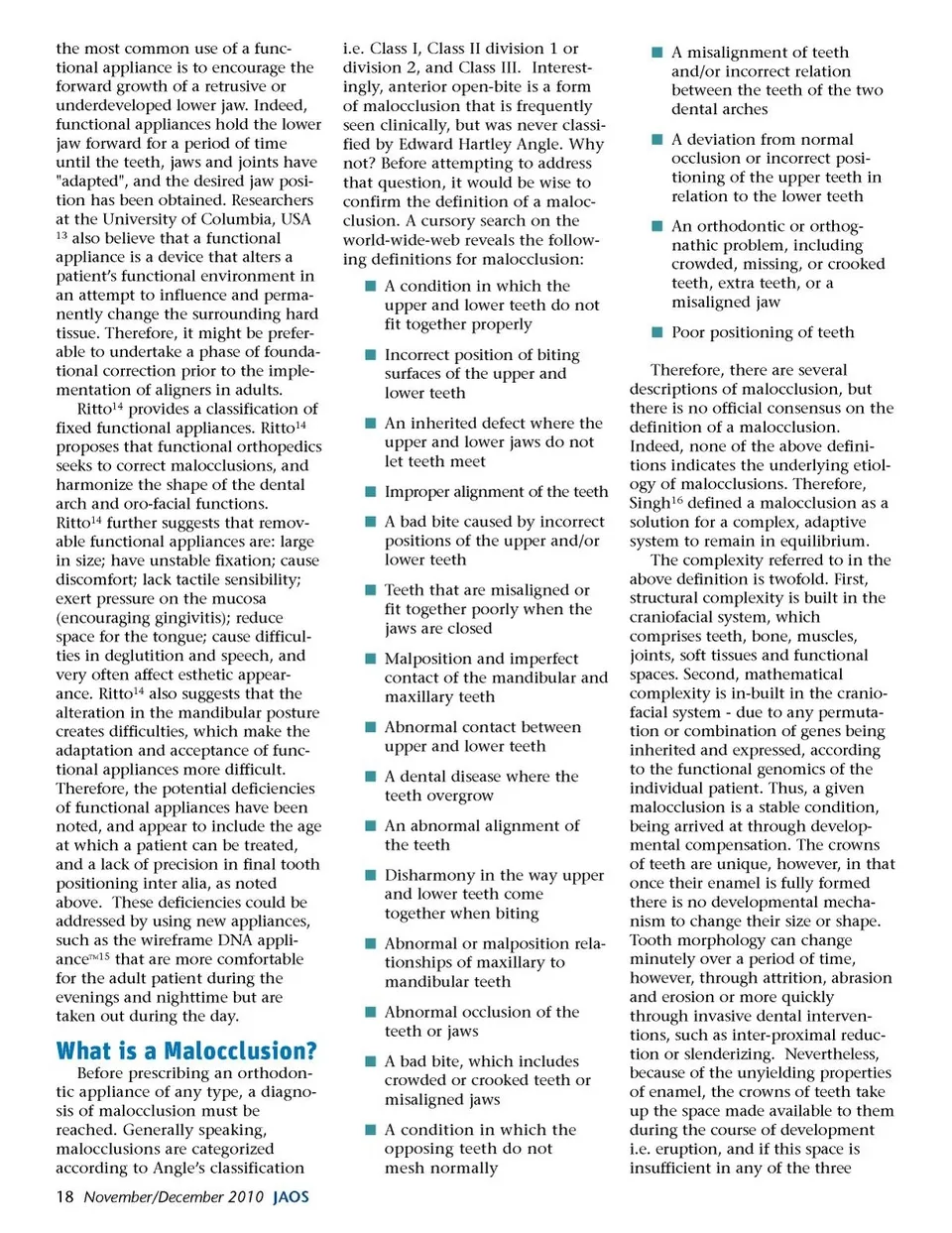
dimensions then a malocclusion arises. Normally, due to temporo-spatial patterning, and given appro-priate gene-environmental interac-tions, teeth will align themselves following the curves of Monson and Spee because of tooth morphology, which has evolved over millennia, to produce a Class I occlusion. In modern societies, however, altered gene-environmental interactions (e.g. bottle-feeding, digit-sucking etc.) mean that teeth can end up in positions in which they are not optimal in terms of either function or esthetics. Thus, foundational correction could place the teeth close to their optimal functional position while aligners could be used to detail the final esthetics. In addition to complexity, however, the craniofacial system has adaptability. The framework of the jaws is built from bone which, due to its rich vascularity, has a high degree of plasticity. This means that the facial skeleton can undergo bone remodeling in response to functional stimuli. Thus, while the teeth are actively erupting, their roots and supporting bone are subject to functional stim-uli, which mold the final outcome. For example, if an object (such as a pacifier, soother or dummy) is placed close to the eruptive path-way, the teeth are in effect deflected into a position different than that determined by temporo-spatial patterning alone. However, the teeth retain their pre-determined morphology while the enclosing bone is ‘deformed’ through remod-eling. This means that the applica-tion of an appropriate signal that remodels the bone can result in the correct re-positioning of the teeth. Thus, both bone morphology and tooth position need to be addressed. Despite the propensity for adapt-ability, the final arbitrator is stabil-ity. The craniofacial system needs to be in balance or equilibrium in accord with functional demands; for example sufficient space for the tongue during sleep, speech, swal-lowing and mastication. Thus, a developmental compromise may be reached with the teeth in a less than ideal position but in a state in which a state of craniofacial home-ostasis has been reached. According to the Spatial Matrix Hypothesis 17 , during growth and development the craniofacial system adapts through developmental compensation until a new position of functional stability has been reached. Moreover, fixed and functional orthodontic appli-ances may modulate this state of developmental stability to the bene-fit (or detriment) of individual patients. Therefore, it is important to aim for improved craniofacial homeostasis and not improved tooth position alone. Spatial Matrix Hypothesis In the recent debate on the etiol-ogy and management of malocclu-sions, it has been noted that maloc-clusions are commonly encountered in modern civilizations, most likely due to changes in environmental conditions, such as feeding behav-ior. Thus, malocclusions might begin at birth, as modern mothers are less likely to breastfeed a child, whereas primitive cultures did so exclusively. Similarly, while the young children of primitive cultures did not ever use pacifiers nor were ever bottle-fed, these recent changes in environment/behavior might be associated with malocclusions such as anterior open-bite, which was so rare even a century ago that Angle omitted this malocclusion from his classification system. Indeed, recent work by Corruccini et al. 18 points to canalization. Put simply, the amount of genetic variance is suppressed or buffered by (canaliz-ing) environmental factors to produce certain outcomes, such as Class I, Class II and Class III maloc-clusions. But, when the environ-mental influences changed, the www.orthodontics.com November/December 2010 19
Journal of the American Orthodontic Society November-December 2010: Page 19