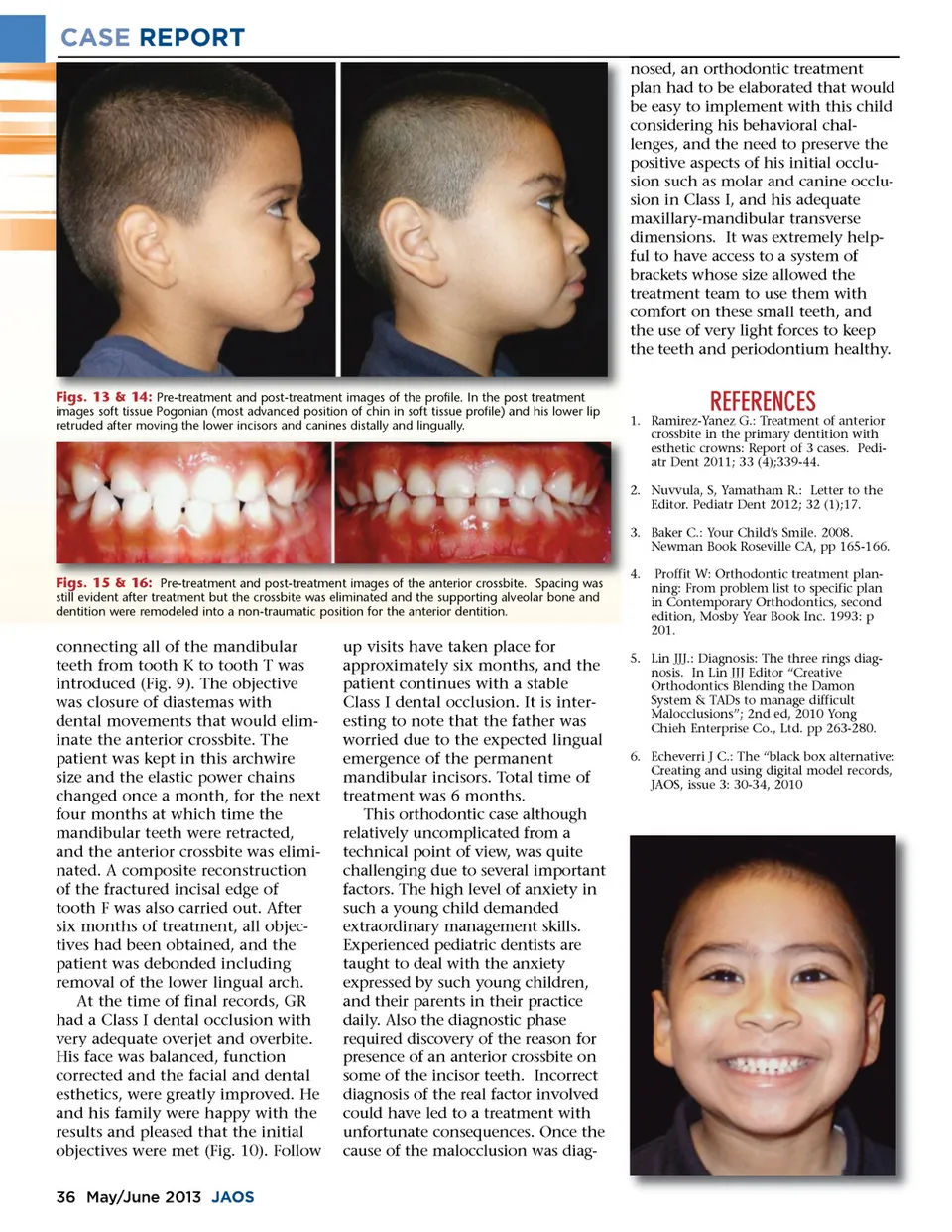
CASE REPORT nosed, an orthodontic treatment plan had to be elaborated that would be easy to implement with this child considering his behavioral chal-lenges, and the need to preserve the positive aspects of his initial occlu-sion such as molar and canine occlu-sion in Class I, and his adequate maxillary-mandibular transverse dimensions. It was extremely help-ful to have access to a system of brackets whose size allowed the treatment team to use them with comfort on these small teeth, and the use of very light forces to keep the teeth and periodontium healthy. Figs. 13 & 14: Pre-treatment and post-treatment images of the profile. In the post treatment images soft tissue Pogonian (most advanced position of chin in soft tissue profile) and his lower lip retruded after moving the lower incisors and canines distally and lingually. 1. Ramirez-Yanez G.: Treatment of anterior crossbite in the primary dentition with esthetic crowns: Report of 3 cases. Pedi-atr Dent 2011; 33 (4);339-44. 2 Nuvvula, S, Yamatham R.: Letter to the 2. Editor. Pediatr Dent 2012; 32 (1);17. 3 Baker C.: Your Child’s Smile. 2008. 3. Newman Book Roseville CA, pp 165-166. REFERENCES Figs. 15 & 16: Pre-treatment and post-treatment images of the anterior crossbite. Spacing was still evident after treatment but the crossbite was eliminated and the supporting alveolar bone and dentition were remodeled into a non-traumatic position for the anterior dentition. 4 4. Proffit W: Orthodontic treatment plan-ning: From problem list to specific plan in Contemporary Orthodontics, second edition, Mosby Year Book Inc. 1993: p 201. connecting all of the mandibular teeth from tooth K to tooth T was introduced (Fig. 9). The objective was closure of diastemas with dental movements that would elim-inate the anterior crossbite. The patient was kept in this archwire size and the elastic power chains changed once a month, for the next four months at which time the mandibular teeth were retracted, and the anterior crossbite was elimi-nated. A composite reconstruction of the fractured incisal edge of tooth F was also carried out. After six months of treatment, all objec-tives had been obtained, and the patient was debonded including removal of the lower lingual arch. At the time of final records, GR had a Class I dental occlusion with very adequate overjet and overbite. His face was balanced, function corrected and the facial and dental esthetics, were greatly improved. He and his family were happy with the results and pleased that the initial objectives were met (Fig. 10). Follow 36 May/June 2013 JAOS up visits have taken place for approximately six months, and the patient continues with a stable Class I dental occlusion. It is inter-esting to note that the father was worried due to the expected lingual emergence of the permanent mandibular incisors. Total time of treatment was 6 months. This orthodontic case although relatively uncomplicated from a technical point of view, was quite challenging due to several important factors. The high level of anxiety in such a young child demanded extraordinary management skills. Experienced pediatric dentists are taught to deal with the anxiety expressed by such young children, and their parents in their practice daily. Also the diagnostic phase required discovery of the reason for presence of an anterior crossbite on some of the incisor teeth. Incorrect diagnosis of the real factor involved could have led to a treatment with unfortunate consequences. Once the cause of the malocclusion was diag-5. Lin JJJ.: Diagnosis: The three rings diag-nosis. In Lin JJJ Editor “Creative Orthodontics Blending the Damon System & TADs to manage difficult Malocclusions”; 2nd ed, 2010 Yong Chieh Enterprise Co., Ltd. pp 263-280. 6. Echeverri J C.: The “black box alternative: Creating and using digital model records, JAOS, issue 3: 30-34, 2010
Journal of the American Orthodontic Society May-June 2013: Page 36