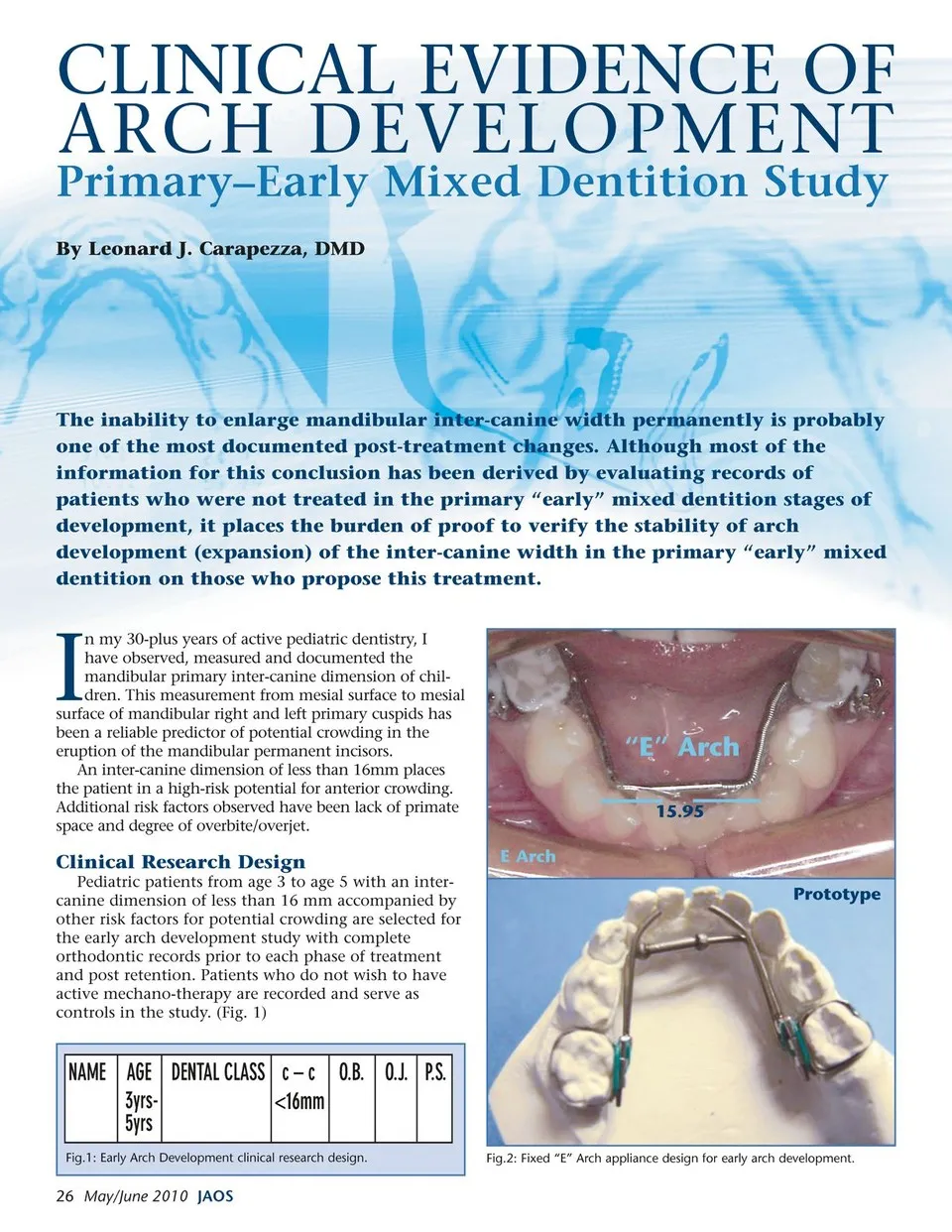
ARCH DEVELOPMENT Primary–Early Mixed Dentition Study By Leonard J. Carapezza, DMD The inability to enlarge mandibular inter-canine width permanently is probably one of the most documented post-treatment changes. Although most of the information for this conclusion has been derived by evaluating records of patients who were not treated in the primary “early” mixed dentition stages of development, it places the burden of proof to verify the stability of arch development (expansion) of the inter-canine width in the primary “early” mixed dentition on those who propose this treatment. I n my 30-plus years of active pediatric dentistry, I have observed, measured and documented the mandibular primary inter-canine dimension of chil- dren. This measurement from mesial surface to mesial surface of mandibular right and left primary cuspids has been a reliable predictor of potential crowding in the eruption of the mandibular permanent incisors. An inter-canine dimension of less than 16mm places the patient in a high-risk potential for anterior crowding. Additional risk factors observed have been lack of primate space and degree of overbite/overjet. Clinical Research Design Pediatric patients from age 3 to age 5 with an inter- canine dimension of less than 16 mm accompanied by other risk factors for potential crowding are selected for the early arch development study with complete orthodontic records prior to each phase of treatment and post retention. Patients who do not wish to have active mechano-therapy are recorded and serve as controls in the study. (Fig. 1) E Arch Prototype CLINICAL EVIDENCE OF “E” Arch 15.95 Fig.1: Early Arch Development clinical research design. 26 May/June 2010 JAOS Fig.2: Fixed “E” Arch appliance design for early arch development.
Journal of the American Orthodontic Society May-June 2010: Page 26