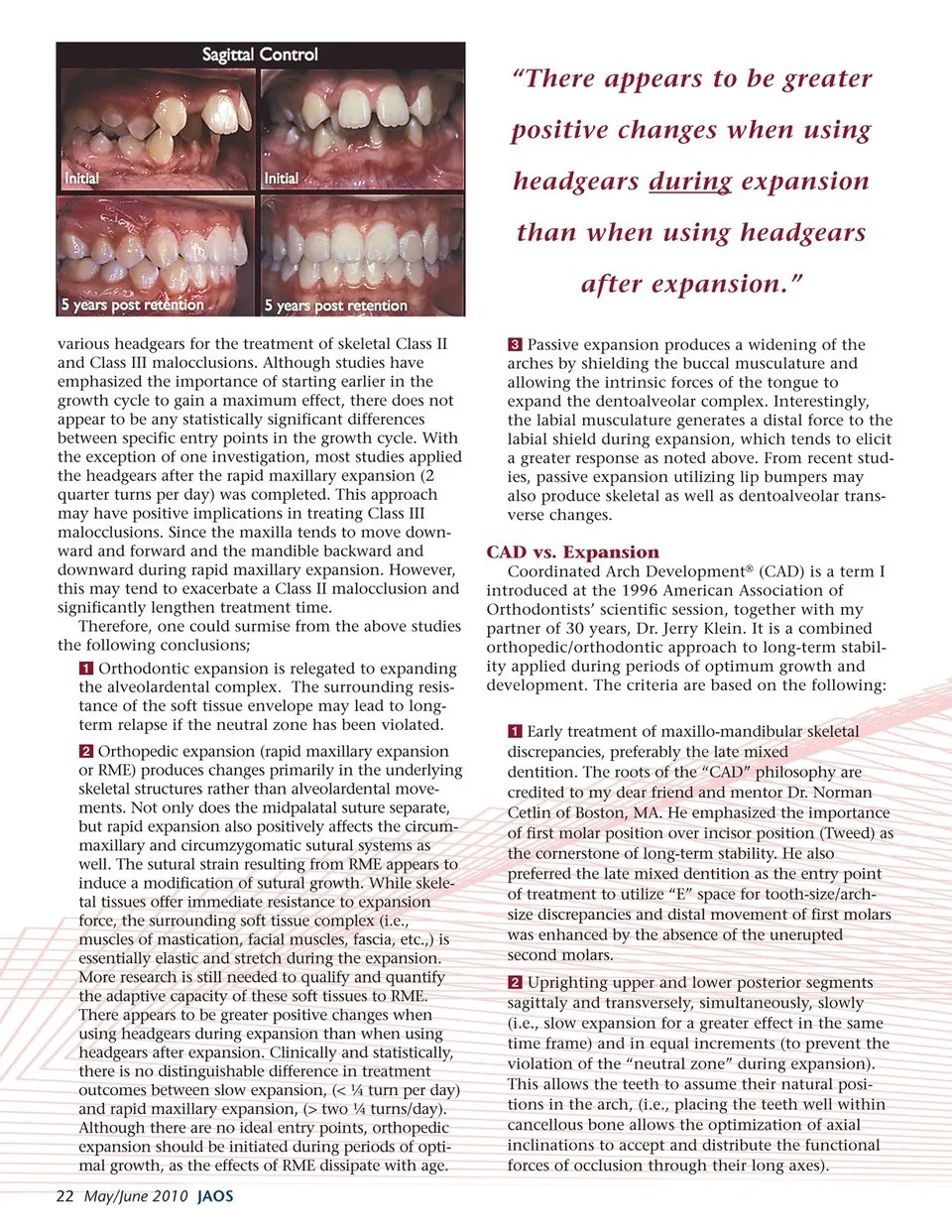
“There appears to be greater positive changes when using headgears during expansion than when using headgears after expansion.” various headgears for the treatment of skeletal Class II and Class III malocclusions. Although studies have emphasized the importance of starting earlier in the growth cycle to gain a maximum effect, there does not appear to be any statistically significant differences between specific entry points in the growth cycle. With the exception of one investigation, most studies applied the headgears after the rapid maxillary expansion (2 quarter turns per day) was completed. This approach may have positive implications in treating Class III malocclusions. Since the maxilla tends to move down- ward and forward and the mandible backward and downward during rapid maxillary expansion. However, this may tend to exacerbate a Class II malocclusion and significantly lengthen treatment time. Therefore, one could surmise from the above studies the following conclusions; Orthodontic expansion is relegated to expanding the alveolardental complex. The surrounding resis- tance of the soft tissue envelope may lead to long- term relapse if the neutral zone has been violated. Orthopedic expansion (rapid maxillary expansion or RME) produces changes primarily in the underlying skeletal structures rather than alveolardental move- ments. Not only does the midpalatal suture separate, but rapid expansion also positively affects the circum- maxillary and circumzygomatic sutural systems as well. The sutural strain resulting from RME appears to induce a modification of sutural growth. While skele- tal tissues offer immediate resistance to expansion force, the surrounding soft tissue complex (i.e., muscles of mastication, facial muscles, fascia, etc.,) is essentially elastic and stretch during the expansion. More research is still needed to qualify and quantify the adaptive capacity of these soft tissues to RME. There appears to be greater positive changes when using headgears during expansion than when using headgears after expansion. Clinically and statistically, there is no distinguishable difference in treatment outcomes between slow expansion, (< ¼ turn per day) and rapid maxillary expansion, (> two ¼ turns/day). Although there are no ideal entry points, orthopedic expansion should be initiated during periods of opti- mal growth, as the effects of RME dissipate with age. 22 May/June 2010 JAOS Passive expansion produces a widening of the arches by shielding the buccal musculature and allowing the intrinsic forces of the tongue to expand the dentoalveolar complex. Interestingly, the labial musculature generates a distal force to the labial shield during expansion, which tends to elicit a greater response as noted above. From recent stud- ies, passive expansion utilizing lip bumpers may also produce skeletal as well as dentoalveolar trans- verse changes. CAD vs. Expansion Coordinated Arch Development® (CAD) is a term I introduced at the 1996 American Association of Orthodontists’ scientific session, together with my partner of 30 years, Dr. Jerry Klein. It is a combined orthopedic/orthodontic approach to long-term stabil- ity applied during periods of optimum growth and development. The criteria are based on the following: Early treatment of maxillo-mandibular skeletal discrepancies, preferably the late mixed dentition. The roots of the “CAD” philosophy are credited to my dear friend and mentor Dr. Norman Cetlin of Boston, MA. He emphasized the importance of first molar position over incisor position (Tweed) as the cornerstone of long-term stability. He also preferred the late mixed dentition as the entry point of treatment to utilize “E” space for tooth-size/arch- size discrepancies and distal movement of first molars was enhanced by the absence of the unerupted second molars. Uprighting upper and lower posterior segments sagittaly and transversely, simultaneously, slowly (i.e., slow expansion for a greater effect in the same time frame) and in equal increments (to prevent the violation of the “neutral zone” during expansion). This allows the teeth to assume their natural posi- tions in the arch, (i.e., placing the teeth well within cancellous bone allows the optimization of axial inclinations to accept and distribute the functional forces of occlusion through their long axes).
Journal of the American Orthodontic Society May-June 2010: Page 22