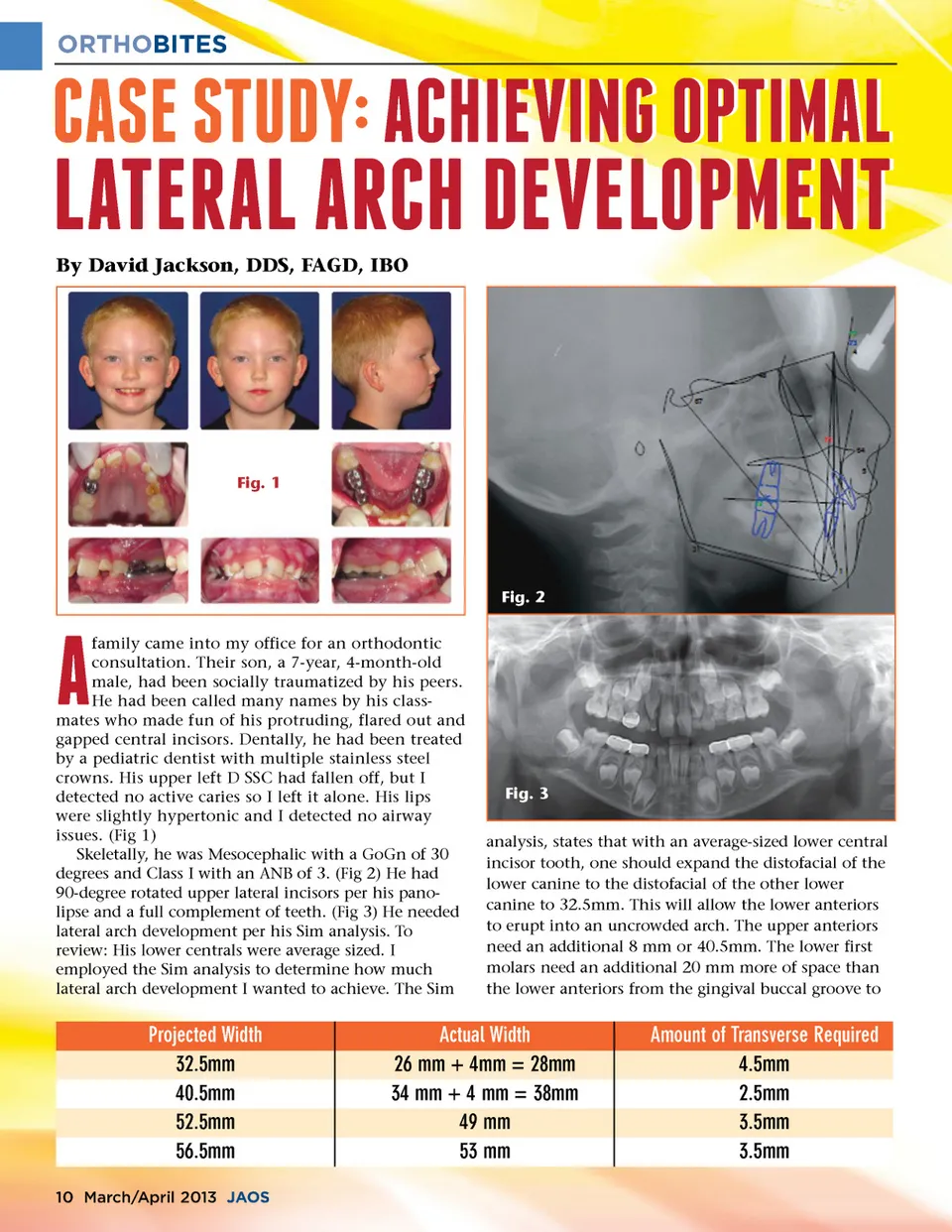
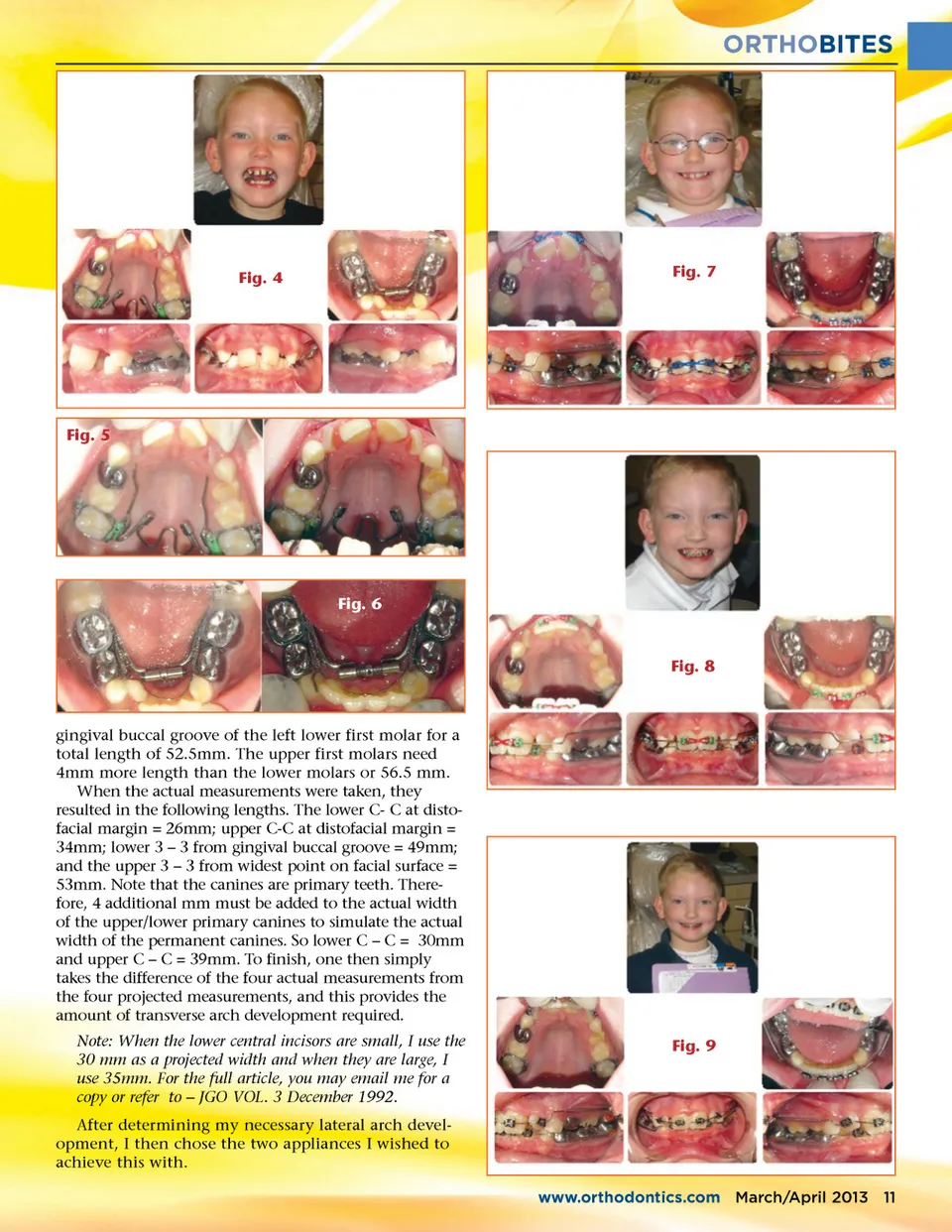
ORTHOBITES e;#�f;"2�f;!  e;#�f;"2�f;! 2#e; d;"d;�d;2 �e;!d;#f; #e; d;"d;�d;2 �e;!d;#f; By David Jackson, DDS, FAGD, IBO f;#!"#f;2#e; 2""f; �e;"! Fig. 1 Fig. 2 # family came into my office for an orthodontic consultation. Their son, a 7-year, 4-month-old male, had been socially traumatized by his peers. He had been called many names by his class-mates who made fun of his protruding, flared out and gapped central incisors. Dentally, he had been treated by a pediatric dentist with multiple stainless steel crowns. His upper left D SSC had fallen off, but I detected no active caries so I left it alone. His lips were slightly hypertonic and I detected no airway issues. (Fig 1) Skeletally, he was Mesocephalic with a GoGn of 30 degrees and Class I with an ANB of 3. (Fig 2) He had 90-degree rotated upper lateral incisors per his pano-lipse and a full complement of teeth. (Fig 3) He needed lateral arch development per his Sim analysis. To review: His lower centrals were average sized. I employed the Sim analysis to determine how much lateral arch development I wanted to achieve. The Sim Fig. 3 analysis, states that with an average-sized lower central incisor tooth, one should expand the distofacial of the lower canine to the distofacial of the other lower canine to 32.5mm. This will allow the lower anteriors to erupt into an uncrowded arch. The upper anteriors need an additional 8 mm or 40.5mm. The lower first molars need an additional 20 mm more of space than the lower anteriors from the gingival buccal groove to Projected Width 32.5mm 40.5mm 52.5mm 56.5mm 10 March/April 2013 JAOS Actual Width 26 mm + 4mm = 28mm 34 mm + 4 mm = 38mm 49 mm 53 mm Amount of Transverse Required 4.5mm 2.5mm 3.5mm 3.5mm
Journal of the American Orthodontic Society March-April 2013: Page 10