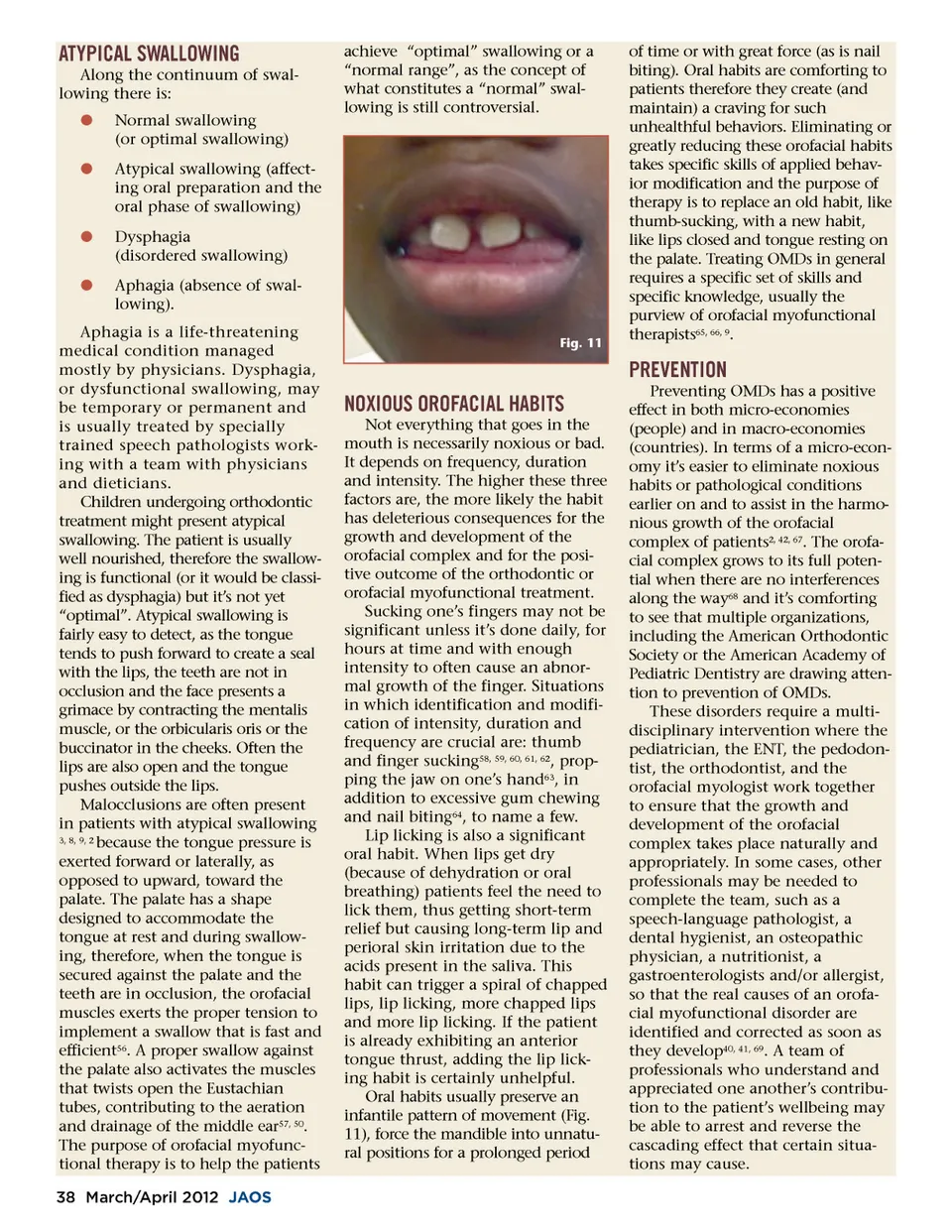
ATYPICAL SWALLOWING Along the continuum of swal-lowing there is: b b Normal swallowing (or optimal swallowing) Atypical swallowing (affect-ing oral preparation and the oral phase of swallowing) Dysphagia (disordered swallowing) Aphagia (absence of swal-lowing). achieve “optimal” swallowing or a “normal range”, as the concept of what constitutes a “normal” swal-lowing is still controversial. b b Aphagia is a life-threatening medical condition managed mostly by physicians. Dysphagia, or dysfunctional swallowing, may be temporary or permanent and is usually treated by specially trained speech pathologists work-ing with a team with physicians and dieticians. Children undergoing orthodontic treatment might present atypical swallowing. The patient is usually well nourished, therefore the swallow-ing is functional (or it would be classi-fied as dysphagia) but it’s not yet “optimal”. Atypical swallowing is fairly easy to detect, as the tongue tends to push forward to create a seal with the lips, the teeth are not in occlusion and the face presents a grimace by contracting the mentalis muscle, or the orbicularis oris or the buccinator in the cheeks. Often the lips are also open and the tongue pushes outside the lips. Malocclusions are often present in patients with atypical swallowing 3, 8, 9, 2 because the tongue pressure is exerted forward or laterally, as opposed to upward, toward the palate. The palate has a shape designed to accommodate the tongue at rest and during swallow-ing, therefore, when the tongue is secured against the palate and the teeth are in occlusion, the orofacial muscles exerts the proper tension to implement a swallow that is fast and efficient 56 . A proper swallow against the palate also activates the muscles that twists open the Eustachian tubes, contributing to the aeration and drainage of the middle ear 57, 50 . The purpose of orofacial myofunc-tional therapy is to help the patients 38 March/April 2012 JAOS Fig. 11 of time or with great force (as is nail biting). Oral habits are comforting to patients therefore they create (and maintain) a craving for such unhealthful behaviors. Eliminating or greatly reducing these orofacial habits takes specific skills of applied behav-ior modification and the purpose of therapy is to replace an old habit, like thumb-sucking, with a new habit, like lips closed and tongue resting on the palate. Treating OMDs in general requires a specific set of skills and specific knowledge, usually the purview of orofacial myofunctional therapists 65, 66, 9 . PREVENTION NOXIOUS OROFACIAL HABITS Not everything that goes in the mouth is necessarily noxious or bad. It depends on frequency, duration and intensity. The higher these three factors are, the more likely the habit has deleterious consequences for the growth and development of the orofacial complex and for the posi-tive outcome of the orthodontic or orofacial myofunctional treatment. Sucking one’s fingers may not be significant unless it’s done daily, for hours at time and with enough intensity to often cause an abnor-mal growth of the finger. Situations in which identification and modifi-cation of intensity, duration and frequency are crucial are: thumb and finger sucking 58, 59, 60, 61, 62 , prop-ping the jaw on one’s hand 63 , in addition to excessive gum chewing and nail biting 64 , to name a few. Lip licking is also a significant oral habit. When lips get dry (because of dehydration or oral breathing) patients feel the need to lick them, thus getting short-term relief but causing long-term lip and perioral skin irritation due to the acids present in the saliva. This habit can trigger a spiral of chapped lips, lip licking, more chapped lips and more lip licking. If the patient is already exhibiting an anterior tongue thrust, adding the lip lick-ing habit is certainly unhelpful. Oral habits usually preserve an infantile pattern of movement (Fig. 11), force the mandible into unnatu-ral positions for a prolonged period Preventing OMDs has a positive effect in both micro-economies (people) and in macro-economies (countries). In terms of a micro-econ-omy it’s easier to eliminate noxious habits or pathological conditions earlier on and to assist in the harmo-nious growth of the orofacial complex of patients 2, 42, 67 . The orofa-cial complex grows to its full poten-tial when there are no interferences along the way 68 and it’s comforting to see that multiple organizations, including the American Orthodontic Society or the American Academy of Pediatric Dentistry are drawing atten-tion to prevention of OMDs. These disorders require a multi-disciplinary intervention where the pediatrician, the ENT, the pedodon-tist, the orthodontist, and the orofacial myologist work together to ensure that the growth and development of the orofacial complex takes place naturally and appropriately. In some cases, other professionals may be needed to complete the team, such as a speech-language pathologist, a dental hygienist, an osteopathic physician, a nutritionist, a gastroenterologists and/or allergist, so that the real causes of an orofa-cial myofunctional disorder are identified and corrected as soon as they develop 40, 41, 69 . A team of professionals who understand and appreciated one another’s contribu-tion to the patient’s wellbeing may be able to arrest and reverse the cascading effect that certain situa-tions may cause.
Journal of the American Orthodontic Society March-April 2012: Page 38