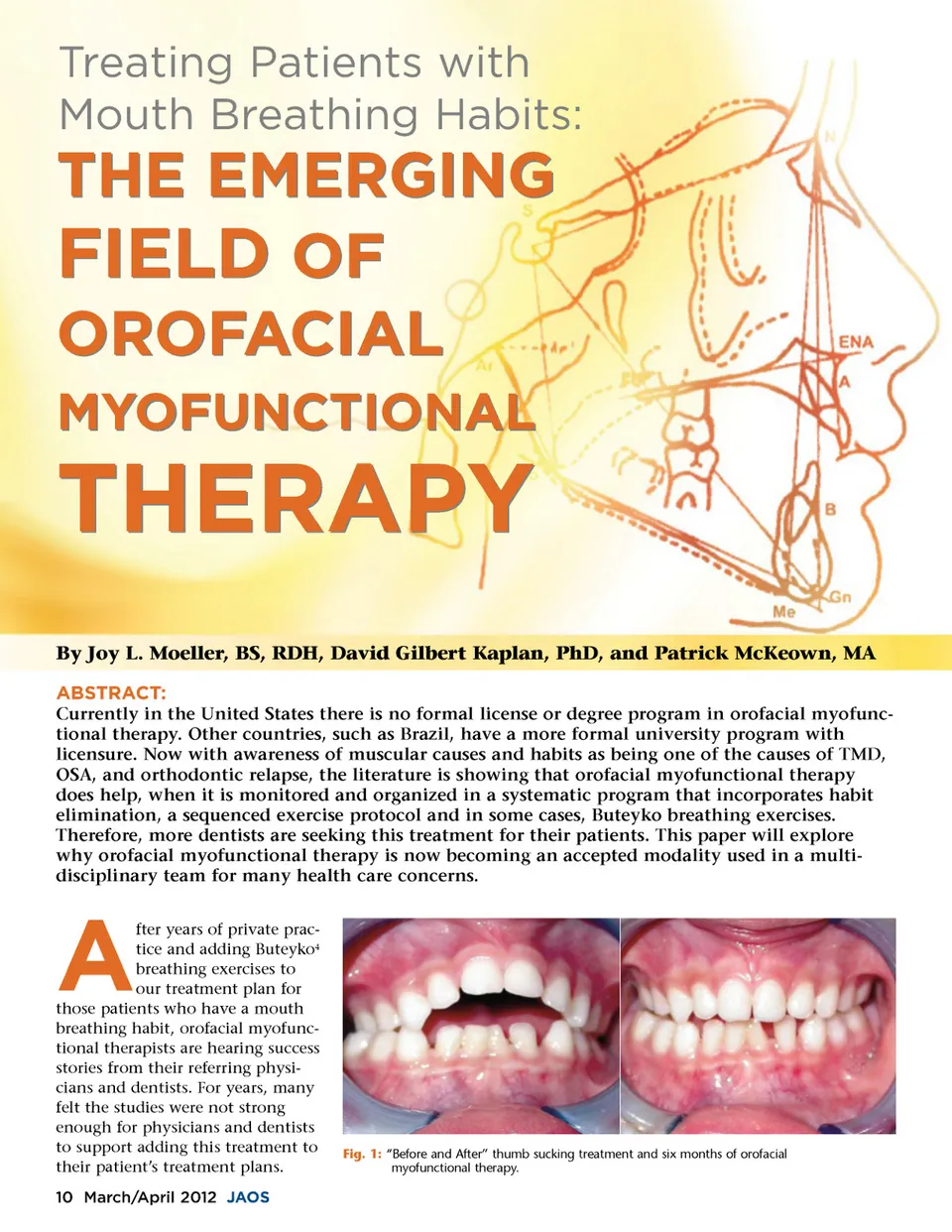
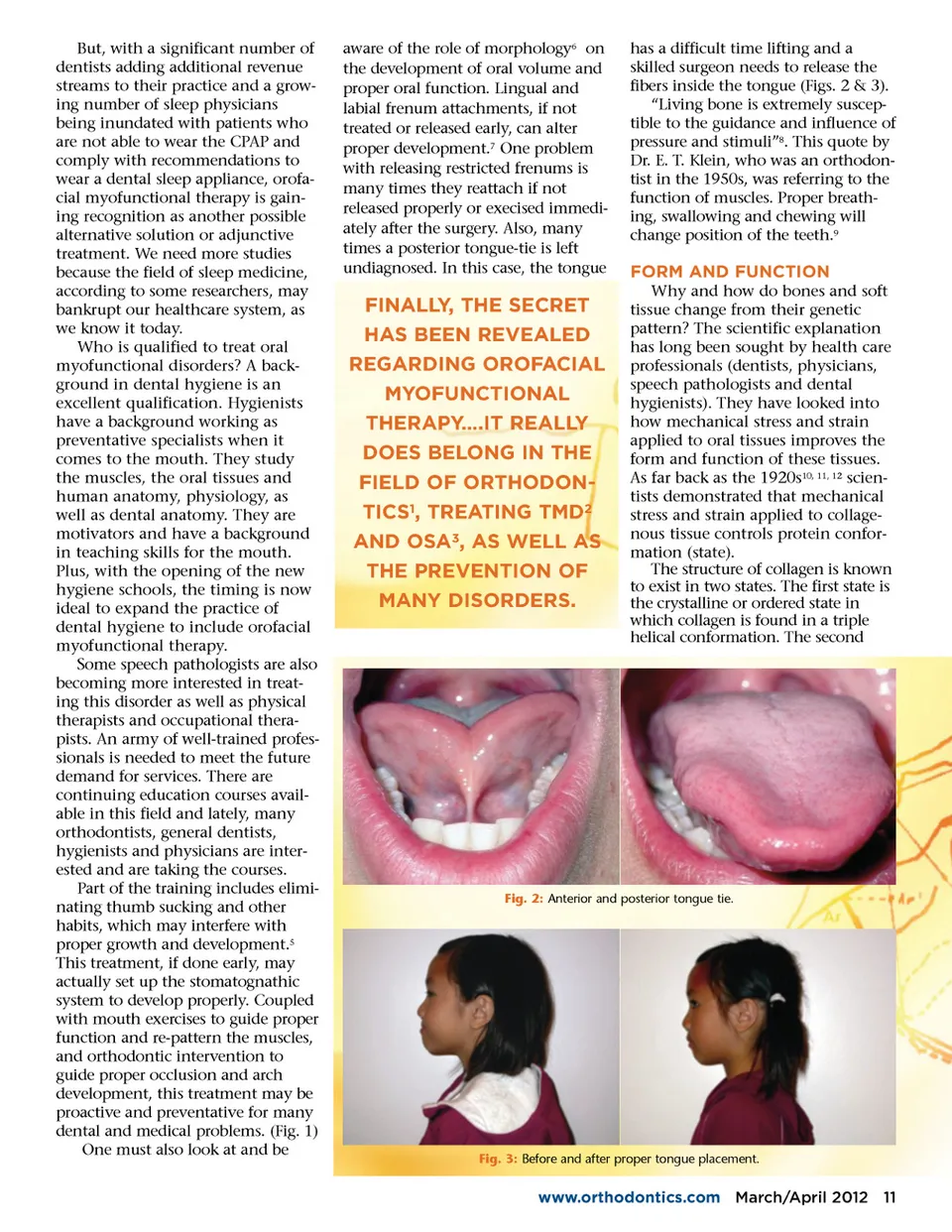
But, with a significant number of dentists adding additional revenue streams to their practice and a grow-ing number of sleep physicians being inundated with patients who are not able to wear the CPAP and comply with recommendations to wear a dental sleep appliance, orofa-cial myofunctional therapy is gain-ing recognition as another possible alternative solution or adjunctive treatment. We need more studies because the field of sleep medicine, according to some researchers, may bankrupt our healthcare system, as we know it today. Who is qualified to treat oral myofunctional disorders? A back-ground in dental hygiene is an excellent qualification. Hygienists have a background working as preventative specialists when it comes to the mouth. They study the muscles, the oral tissues and human anatomy, physiology, as well as dental anatomy. They are motivators and have a background in teaching skills for the mouth. Plus, with the opening of the new hygiene schools, the timing is now ideal to expand the practice of dental hygiene to include orofacial myofunctional therapy. Some speech pathologists are also becoming more interested in treat-ing this disorder as well as physical therapists and occupational thera-pists. An army of well-trained profes-sionals is needed to meet the future demand for services. There are continuing education courses avail-able in this field and lately, many orthodontists, general dentists, hygienists and physicians are inter-ested and are taking the courses. Part of the training includes elimi-nating thumb sucking and other habits, which may interfere with proper growth and development. 5 This treatment, if done early, may actually set up the stomatognathic system to develop properly. Coupled with mouth exercises to guide proper function and re-pattern the muscles, and orthodontic intervention to guide proper occlusion and arch development, this treatment may be proactive and preventative for many dental and medical problems. (Fig. 1) One must also look at and be aware of the role of morphology 6 on the development of oral volume and proper oral function. Lingual and labial frenum attachments, if not treated or released early, can alter proper development. 7 One problem with releasing restricted frenums is many times they reattach if not released properly or execised immedi-ately after the surgery. Also, many times a posterior tongue-tie is left undiagnosed. In this case, the tongue has a difficult time lifting and a skilled surgeon needs to release the fibers inside the tongue (Figs. 2 & 3). “Living bone is extremely suscep-tible to the guidance and influence of pressure and stimuli” 8 . This quote by Dr. E. T. Klein, who was an orthodon-tist in the 1950s, was referring to the function of muscles. Proper breath-ing, swallowing and chewing will change position of the teeth. 9 FORM AND FUNCTION Why and how do bones and soft tissue change from their genetic pattern? The scientific explanation has long been sought by health care professionals (dentists, physicians, speech pathologists and dental hygienists). They have looked into how mechanical stress and strain applied to oral tissues improves the form and function of these tissues. As far back as the 1920s 10, 11, 12 scien-tists demonstrated that mechanical stress and strain applied to collage-nous tissue controls protein confor-mation (state). The structure of collagen is known to exist in two states. The first state is the crystalline or ordered state in which collagen is found in a triple helical conformation. The second FINALLY, THE SECRET HAS BEEN REVEALED REGARDING OROFACIAL MYOFUNCTIONAL THERAPY….IT REALLY DOES BELONG IN THE FIELD OF ORTHODON-TICS 1 , TREATING TMD 2 AND OSA 3 , AS WELL AS THE PREVENTION OF MANY DISORDERS. Fig. 2: Anterior and posterior tongue tie. Fig. 3: Before and after proper tongue placement. www.orthodontics.com March/April 2012 11
Journal of the American Orthodontic Society March-April 2012: Page 11