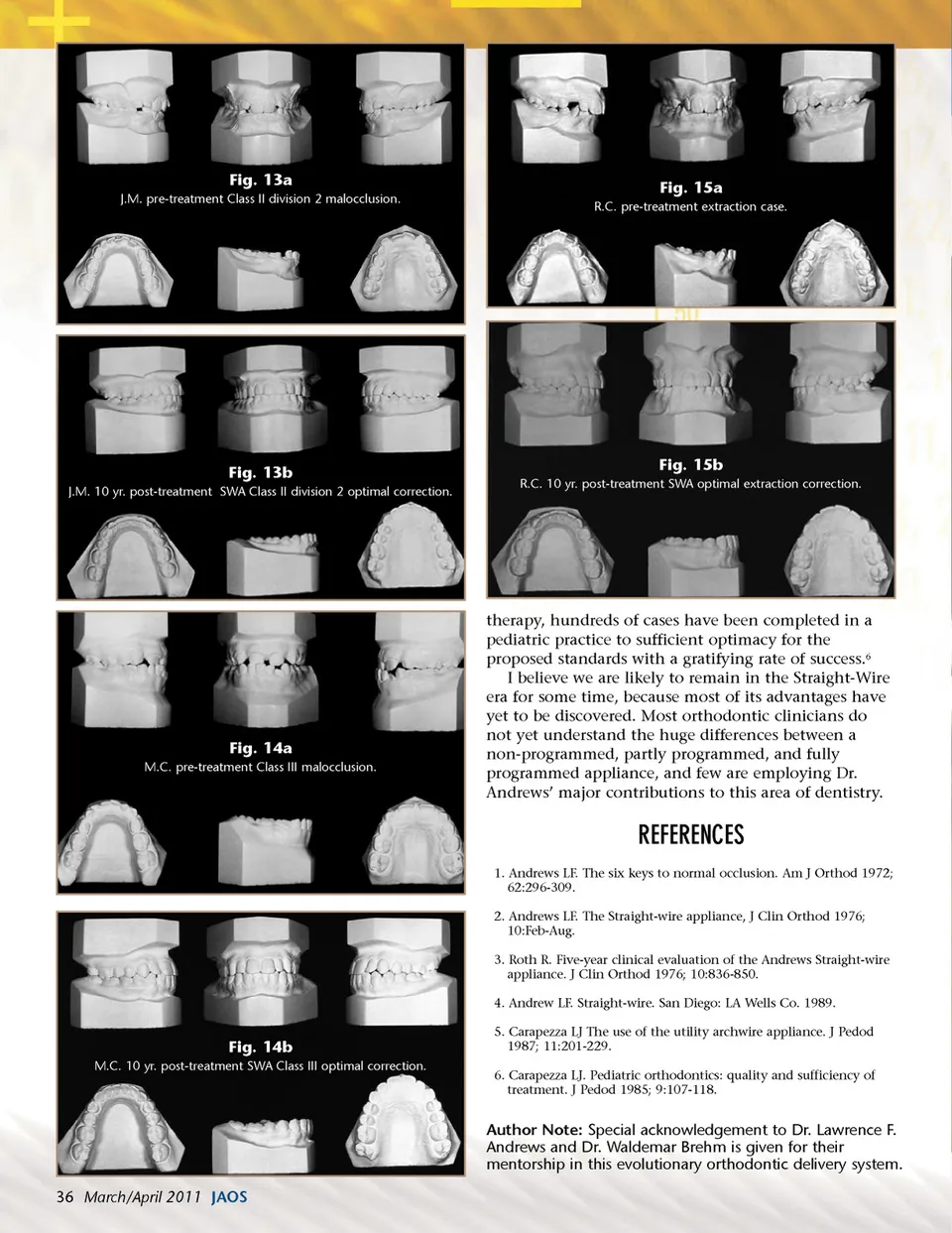
Fig. 13a J.M. pre-treatment Class II division 2 malocclusion. Fig. 15a R.C. pre-treatment extraction case. Fig. 13b J.M. 10 yr. post-treatment SWA Class II division 2 optimal correction. Fig. 15b R.C. 10 yr. post-treatment SWA optimal extraction correction. Fig. 14a M.C. pre-treatment Class III malocclusion. therapy, hundreds of cases have been completed in a pediatric practice to sufficient optimacy for the proposed standards with a gratifying rate of success. 6 I believe we are likely to remain in the Straight-Wire era for some time, because most of its advantages have yet to be discovered. Most orthodontic clinicians do not yet understand the huge differences between a non-programmed, partly programmed, and fully programmed appliance, and few are employing Dr. Andrews’ major contributions to this area of dentistry. REFERENCES 1. Andrews LF. The six keys to normal occlusion. Am J Orthod 1972; 62:296-309. 2. Andrews LF. The Straight-wire appliance, J Clin Orthod 1976; 10:Feb-Aug. 3. Roth R. Five-year clinical evaluation of the Andrews Straight-wire appliance. J Clin Orthod 1976; 10:836-850. 4. Andrew LF. Straight-wire. San Diego: LA Wells Co. 1989. Fig. 14b M.C. 10 yr. post-treatment SWA Class III optimal correction. 5. Carapezza LJ The use of the utility archwire appliance. J Pedod 1987; 11:201-229. 6. Carapezza LJ. Pediatric orthodontics: quality and sufficiency of treatment. J Pedod 1985; 9:107-118. Author Note: Special acknowledgement to Dr. Lawrence F. Andrews and Dr. Waldemar Brehm is given for their mentorship in this evolutionary orthodontic delivery system. 36 March/April 2011 JAOS
Journal of the American Orthodontic Society March-April 2011: Page 36