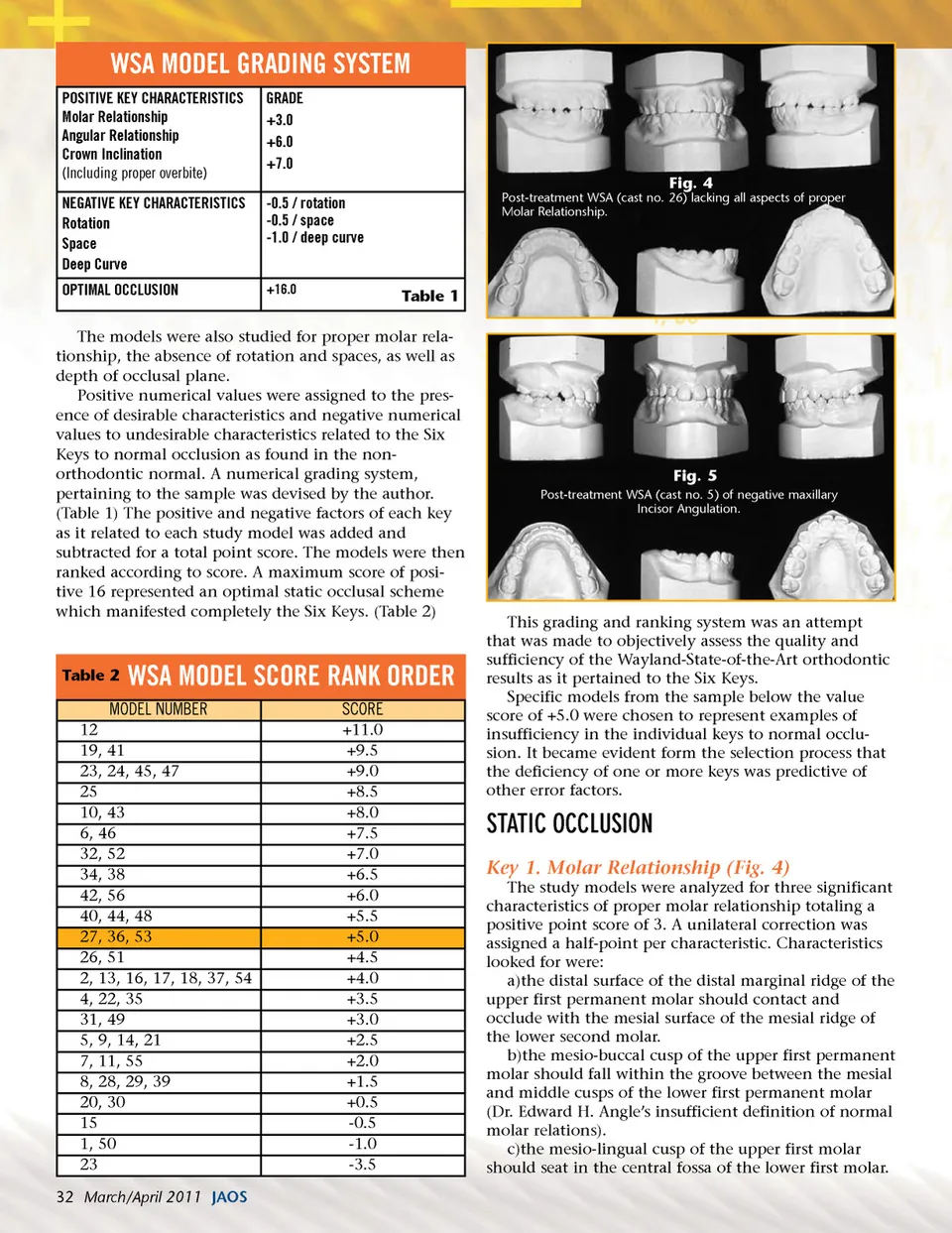
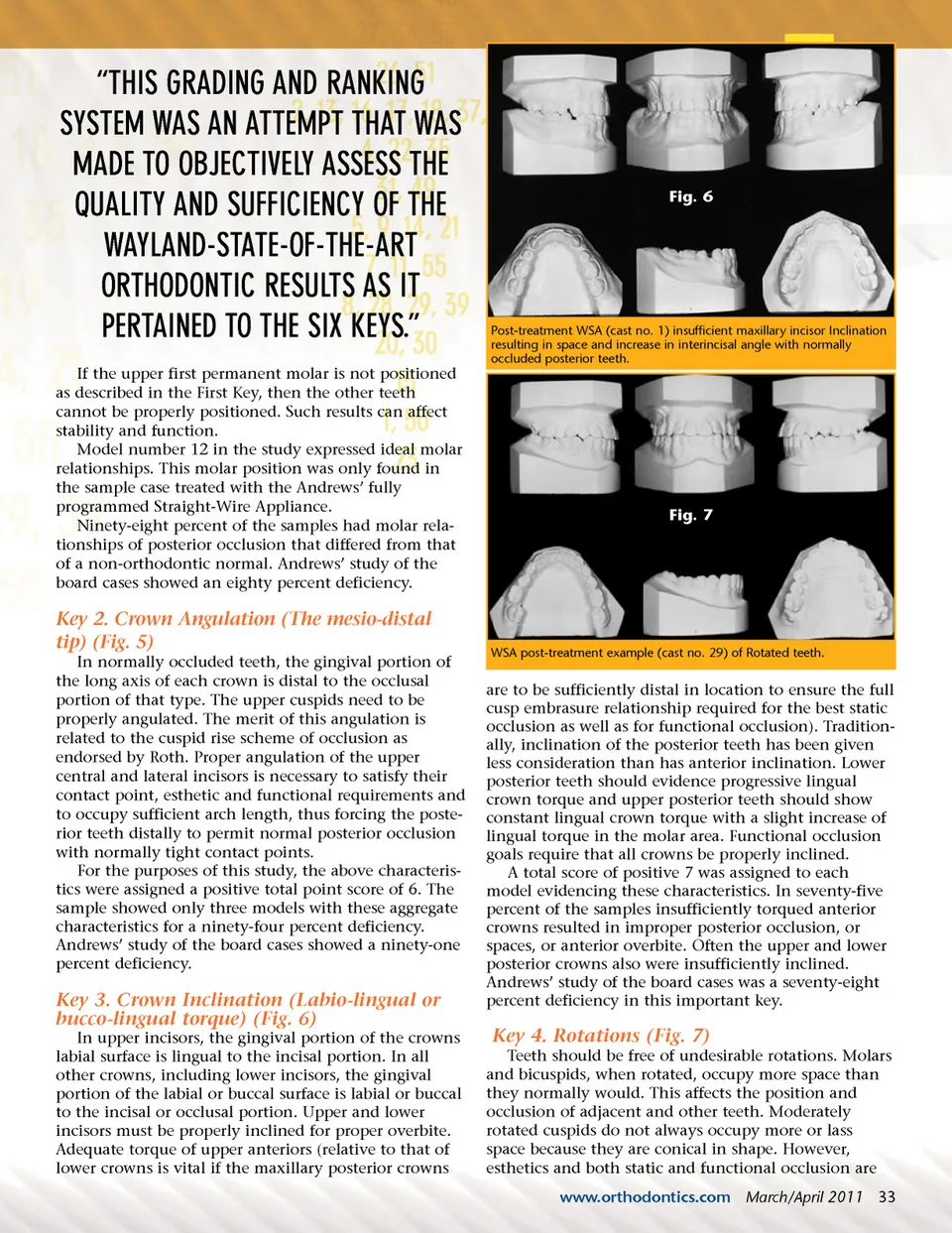
“THIS GRADING AND RANKING SYSTEM WAS AN ATTEMPT THAT WAS MADE TO OBJECTIVELY ASSESS THE QUALITY AND SUFFICIENCY OF THE WAYLAND-STATE-OF-THE-ART ORTHODONTIC RESULTS AS IT PERTAINED TO THE SIX KEYS.” If the upper first permanent molar is not positioned as described in the First Key, then the other teeth cannot be properly positioned. Such results can affect stability and function. Model number 12 in the study expressed ideal molar relationships. This molar position was only found in the sample case treated with the Andrews’ fully programmed Straight-Wire Appliance. Ninety-eight percent of the samples had molar rela-tionships of posterior occlusion that differed from that of a non-orthodontic normal. Andrews’ study of the board cases showed an eighty percent deficiency. Fig. 6 Post-treatment WSA (cast no. 1) insufficient maxillary incisor Inclination resulting in space and increase in interincisal angle with normally occluded posterior teeth. Fig. 7 Key 2. Crown Angulation (The mesio-distal tip) (Fig. 5) In normally occluded teeth, the gingival portion of the long axis of each crown is distal to the occlusal portion of that type. The upper cuspids need to be properly angulated. The merit of this angulation is related to the cuspid rise scheme of occlusion as endorsed by Roth. Proper angulation of the upper central and lateral incisors is necessary to satisfy their contact point, esthetic and functional requirements and to occupy sufficient arch length, thus forcing the poste-rior teeth distally to permit normal posterior occlusion with normally tight contact points. For the purposes of this study, the above characteris-tics were assigned a positive total point score of 6. The sample showed only three models with these aggregate characteristics for a ninety-four percent deficiency. Andrews’ study of the board cases showed a ninety-one percent deficiency. WSA post-treatment example (cast no. 29) of Rotated teeth. Key 3. Crown Inclination (Labio-lingual or bucco-lingual torque) (Fig. 6) In upper incisors, the gingival portion of the crowns labial surface is lingual to the incisal portion. In all other crowns, including lower incisors, the gingival portion of the labial or buccal surface is labial or buccal to the incisal or occlusal portion. Upper and lower incisors must be properly inclined for proper overbite. Adequate torque of upper anteriors (relative to that of lower crowns is vital if the maxillary posterior crowns are to be sufficiently distal in location to ensure the full cusp embrasure relationship required for the best static occlusion as well as for functional occlusion). Tradition-ally, inclination of the posterior teeth has been given less consideration than has anterior inclination. Lower posterior teeth should evidence progressive lingual crown torque and upper posterior teeth should show constant lingual crown torque with a slight increase of lingual torque in the molar area. Functional occlusion goals require that all crowns be properly inclined. A total score of positive 7 was assigned to each model evidencing these characteristics. In seventy-five percent of the samples insufficiently torqued anterior crowns resulted in improper posterior occlusion, or spaces, or anterior overbite. Often the upper and lower posterior crowns also were insufficiently inclined. Andrews’ study of the board cases was a seventy-eight percent deficiency in this important key. Key 4. Rotations (Fig. 7) Teeth should be free of undesirable rotations. Molars and bicuspids, when rotated, occupy more space than they normally would. This affects the position and occlusion of adjacent and other teeth. Moderately rotated cuspids do not always occupy more or lass space because they are conical in shape. However, esthetics and both static and functional occlusion are www.orthodontics.com March/April 2011 33
Journal of the American Orthodontic Society March-April 2011: Page 33