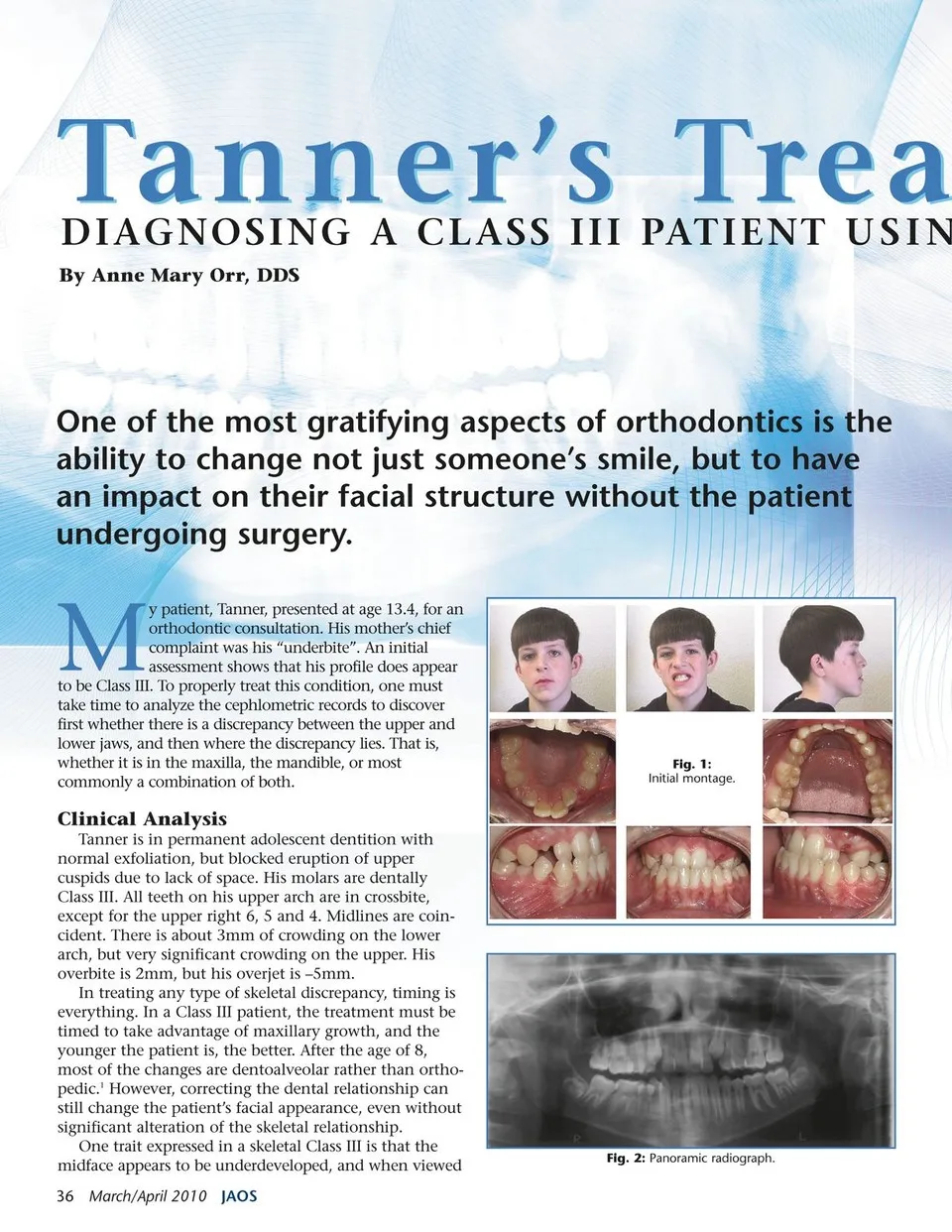
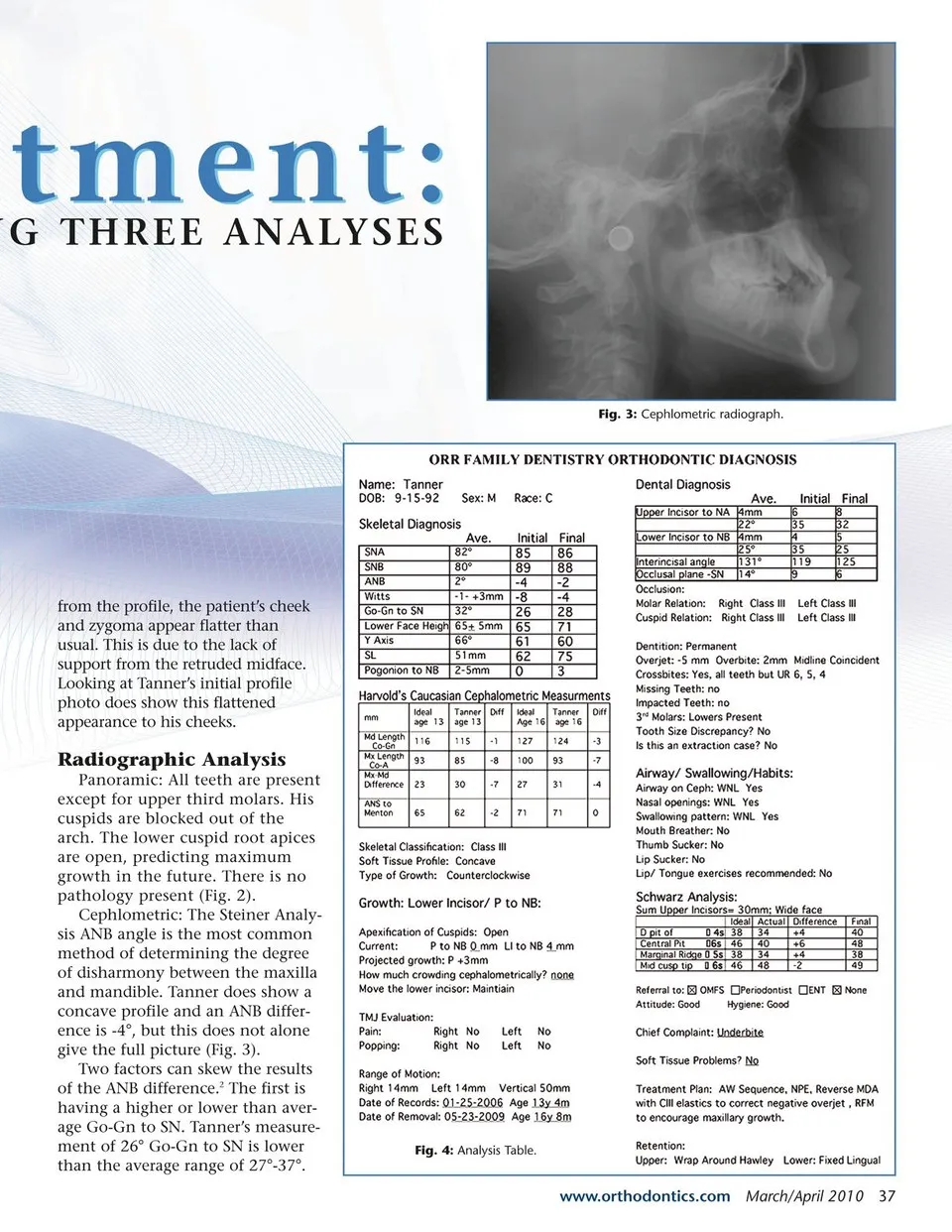
Tanner’s Trea One of the most gratifying aspects of orthodontics is the ability to change not just someone’s smile, but to have an impact on their facial structure without the patient undergoing surgery. M y patient, Tanner, presented at age 13.4, for an orthodontic consultation. His mother’s chief complaint was his “underbite”. An initial assessment shows that his profile does appear to be Class III. To properly treat this condition, one must take time to analyze the cephlometric records to discover first whether there is a discrepancy between the upper and lower jaws, and then where the discrepancy lies. That is, whether it is in the maxilla, the mandible, or most commonly a combination of both. Clinical Analysis Tanner is in permanent adolescent dentition with normal exfoliation, but blocked eruption of upper cuspids due to lack of space. His molars are dentally Class III. All teeth on his upper arch are in crossbite, except for the upper right 6, 5 and 4. Midlines are coin- cident. There is about 3mm of crowding on the lower arch, but very significant crowding on the upper. His overbite is 2mm, but his overjet is –5mm. In treating any type of skeletal discrepancy, timing is everything. In a Class III patient, the treatment must be timed to take advantage of maxillary growth, and the younger the patient is, the better. After the age of 8, most of the changes are dentoalveolar rather than ortho- pedic.1 However, correcting the dental relationship can still change the patient’s facial appearance, even without significant alteration of the skeletal relationship. One trait expressed in a skeletal Class III is that the midface appears to be underdeveloped, and when viewed 36 March/April 2010 JAOS Fig. 2: Panoramic radiograph. DIAGNOSING A CLASS III PATIENT USIN By Anne Mary Orr, DDS Fig. 1: Initial montage.
Journal of the American Orthodontic Society March - April 2010: Page 36