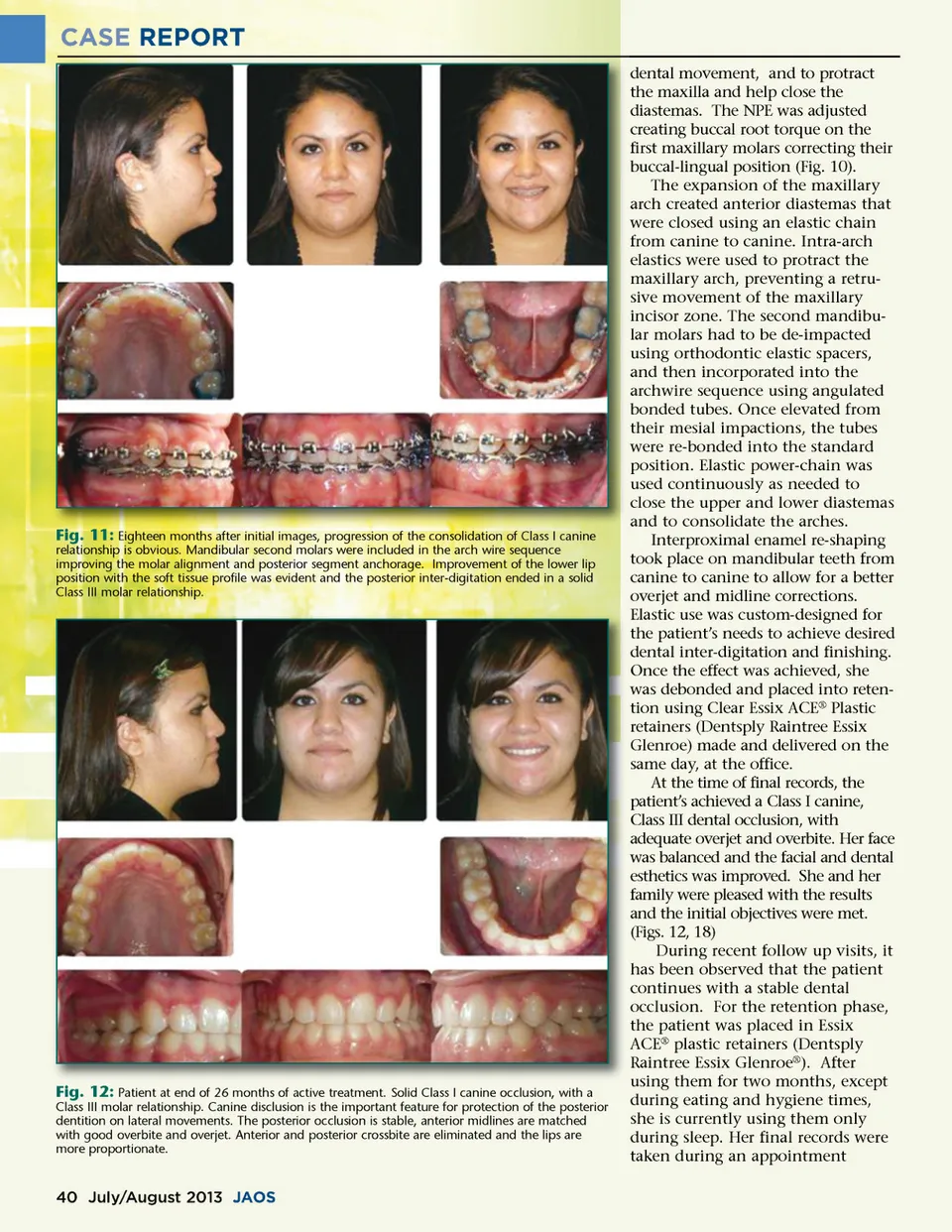
CASE REPORT dental movement, and to protract the maxilla and help close the diastemas. The NPE was adjusted creating buccal root torque on the first maxillary molars correcting their buccal-lingual position (Fig. 10). The expansion of the maxillary arch created anterior diastemas that were closed using an elastic chain from canine to canine. Intra-arch elastics were used to protract the maxillary arch, preventing a retru-sive movement of the maxillary incisor zone. The second mandibu-lar molars had to be de-impacted using orthodontic elastic spacers, and then incorporated into the archwire sequence using angulated bonded tubes. Once elevated from their mesial impactions, the tubes were re-bonded into the standard position. Elastic power-chain was used continuously as needed to close the upper and lower diastemas and to consolidate the arches. Interproximal enamel re-shaping took place on mandibular teeth from canine to canine to allow for a better overjet and midline corrections. Elastic use was custom-designed for the patient’s needs to achieve desired dental inter-digitation and finishing. Once the effect was achieved, she was debonded and placed into reten-tion using Clear Essix ACE ® Plastic retainers (Dentsply Raintree Essix Glenroe) made and delivered on the same day, at the office. At the time of final records, the patient’s achieved a Class I canine, Class III dental occlusion, with adequate overjet and overbite. Her face was balanced and the facial and dental esthetics was improved. She and her family were pleased with the results and the initial objectives were met. (Figs. 12, 18) During recent follow up visits, it has been observed that the patient continues with a stable dental occlusion. For the retention phase, the patient was placed in Essix ACE ® plastic retainers (Dentsply Raintree Essix Glenroe ® ). After using them for two months, except during eating and hygiene times, she is currently using them only during sleep. Her final records were taken during an appointment Fig. 11: Eighteen months after initial images, progression of the consolidation of Class I canine relationship is obvious. Mandibular second molars were included in the arch wire sequence improving the molar alignment and posterior segment anchorage. Improvement of the lower lip position with the soft tissue profile was evident and the posterior inter-digitation ended in a solid Class III molar relationship. Fig. 12: Patient at end of 26 months of active treatment. Solid Class I canine occlusion, with a Class III molar relationship. Canine disclusion is the important feature for protection of the posterior dentition on lateral movements. The posterior occlusion is stable, anterior midlines are matched with good overbite and overjet. Anterior and posterior crossbite are eliminated and the lips are more proportionate. 40 July/August 2013 JAOS
Journal of the American Orthodontic Society July-August 2013 Buyer's Guide: Page 40