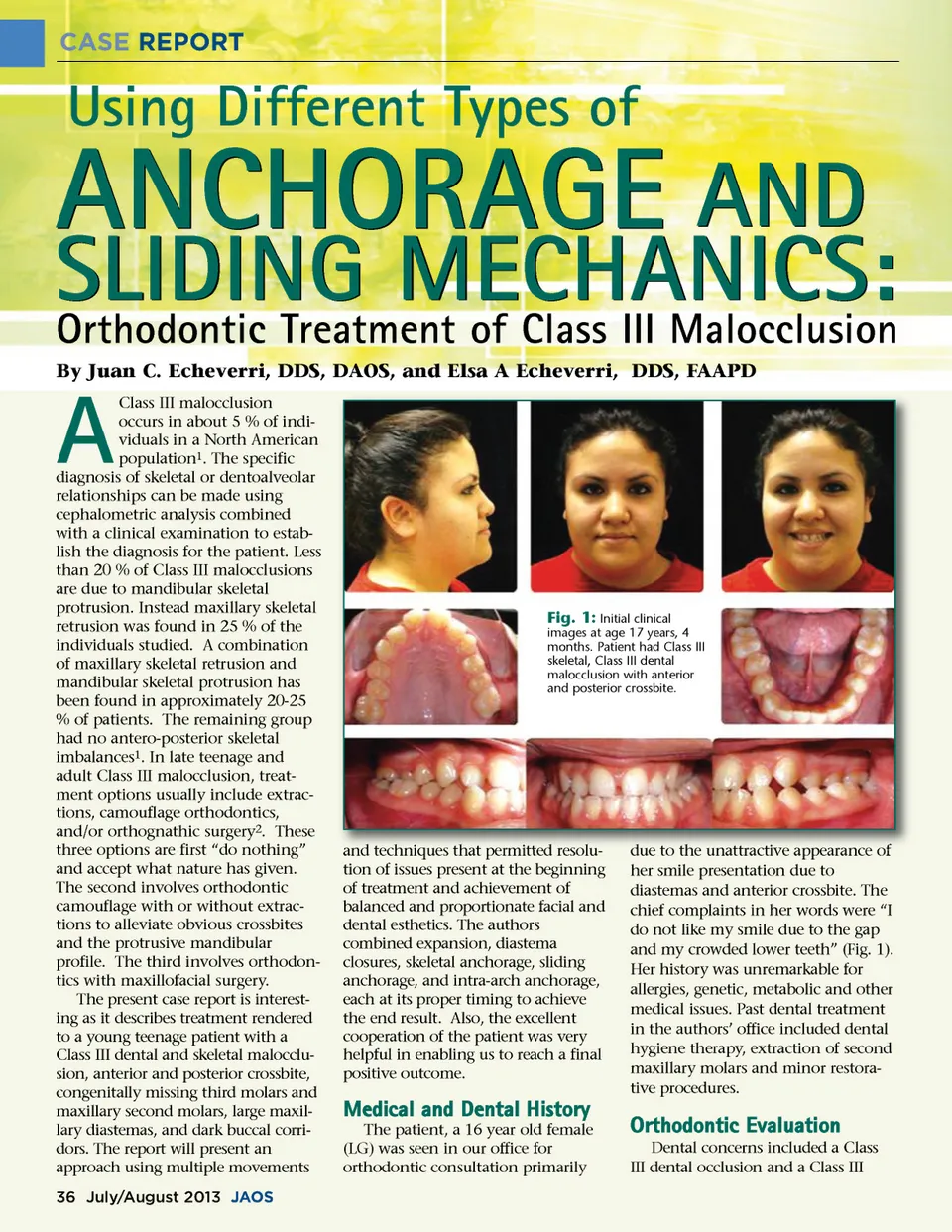
CASE REPORT Using Different Types of ANCHORAGE AND By Juan C. Echeverri, DDS, DAOS, and Elsa A Echeverri, DDS, FAAPD Class III malocclusion occurs in about 5 % of indi-viduals in a North American population 1 . The specific diagnosis of skeletal or dentoalveolar relationships can be made using cephalometric analysis combined with a clinical examination to estab-lish the diagnosis for the patient. Less than 20 % of Class III malocclusions are due to mandibular skeletal protrusion. Instead maxillary skeletal retrusion was found in 25 % of the individuals studied. A combination of maxillary skeletal retrusion and mandibular skeletal protrusion has been found in approximately 20-25 % of patients. The remaining group had no antero-posterior skeletal imbalances 1 . In late teenage and adult Class III malocclusion, treat-ment options usually include extrac-tions, camouflage orthodontics, and/or orthognathic surgery 2 . These three options are first “do nothing” and accept what nature has given. The second involves orthodontic camouflage with or without extrac-tions to alleviate obvious crossbites and the protrusive mandibular profile. The third involves orthodon-tics with maxillofacial surgery. The present case report is interest-ing as it describes treatment rendered to a young teenage patient with a Class III dental and skeletal malocclu-sion, anterior and posterior crossbite, congenitally missing third molars and maxillary second molars, large maxil-lary diastemas, and dark buccal corri-dors. The report will present an approach using multiple movements SLIDING MECHANICS: Orthodontic Treatment of Class III Malocclusion A Fig. 1: Initial clinical images at age 17 years, 4 months. Patient had Class III skeletal, Class III dental malocclusion with anterior and posterior crossbite. and techniques that permitted resolu resolu-tion of issues present at the beginning of treatment and achievement of balanced and proportionate facial and dental esthetics. The authors combined expansion, diastema closures, skeletal anchorage, sliding anchorage, and intra-arch anchorage, each at its proper timing to achieve the end result. Also, the excellent cooperation of the patient was very helpful in enabling us to reach a final positive outcome. due to the unattractive appearance of her smile presentation due to diastemas and anterior crossbite. The chief complaints in her words were “I do not like my smile due to the gap and my crowded lower teeth” (Fig. 1). Her history was unremarkable for allergies, genetic, metabolic and other medical issues. Past dental treatment in the authors’ office included dental hygiene therapy, extraction of second maxillary molars and minor restora-tive procedures. Medical and Dental History The patient, a 16 year old female (LG) was seen in our office for orthodontic consultation primarily Orthodontic Evaluation Dental concerns included a Class III dental occlusion and a Class III 36 July/August 2013 JAOS
Journal of the American Orthodontic Society July-August 2013 Buyer's Guide: Page 36