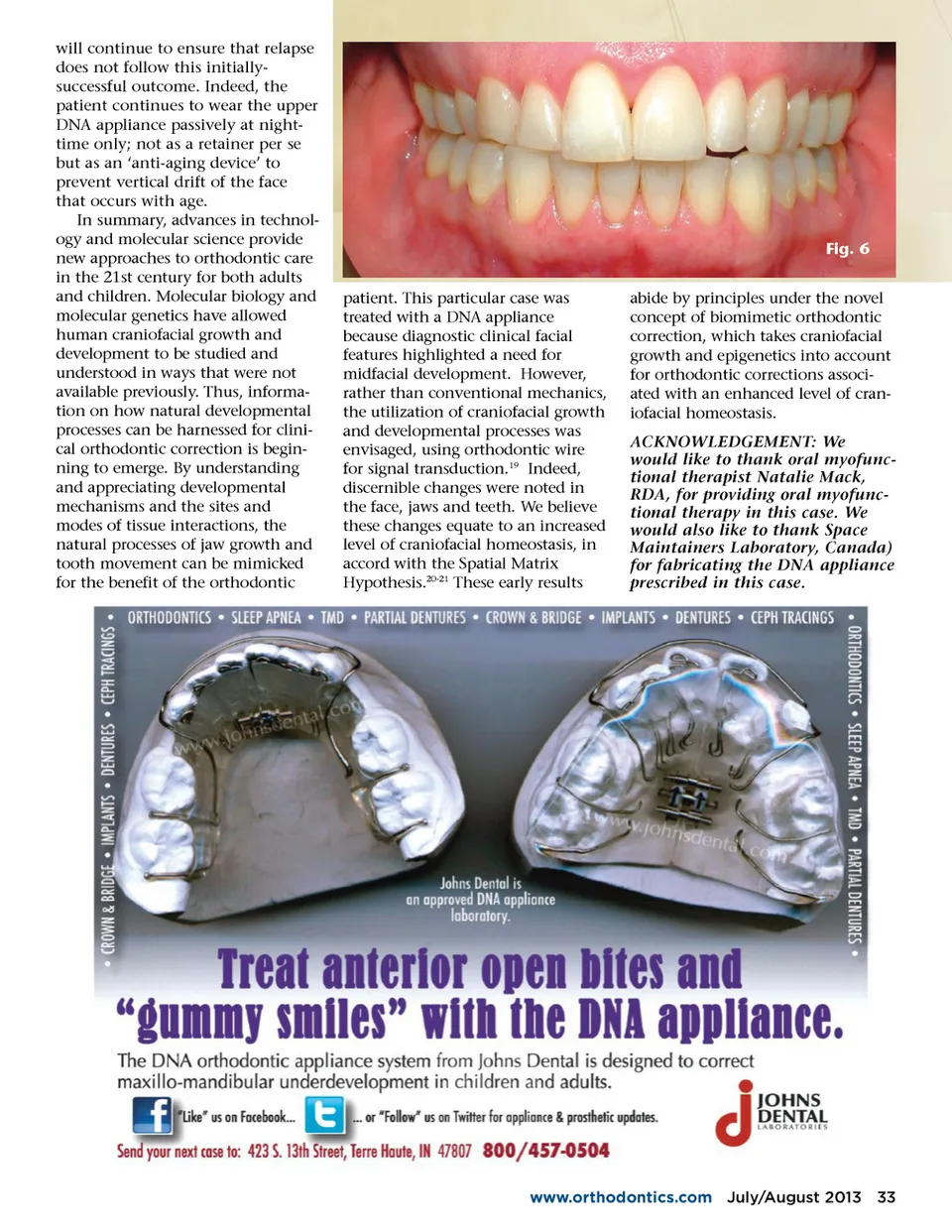
Fig. 4 Fig. 5 occlusion goals, which included anterior coupling. In this case, Speed brackets (Speed System Orthodontics, Cambridge, ON, Canada) were used in the follow-ing wire sequence: 0.014, 0.016, 0.018 with vertical elastics. The duration of fixed appliance ther-apy was 8 months in total. The patient was also instructed in OMT to train the tongue, following a routine prescribed by a trained oral myofunctional therapist. This routine consisted of a series of exer-cises to retrain the tongue to rest in the roof of the mouth. It also encouraged a lips-together posture, and promoted breathing through the nose while at rest. “This particular case was treated with a DNA appliance because diagnostic clinical facial features highlighted a need for midfacial development.” DISCUSSION The human genome has been sequenced, and we now know that certain genes are involved in remodeling bone 1 , tooth develop-ment 7 and tooth eruption. 8 Teeth are naturally-designed to move; for example, tooth eruption in a normally-growing child. In addi-tion, the teeth in some people erupt in a specific arrangement, produc-ing a beautiful smile. The unique arrangement of teeth is due to homeobox genes 9 that help produce an ideal bone morphology. In fact, a natural process called 'temporo-spatial patterning' is at work. 10 This process can be regarded as a blueprint or body plan that is encoded by genes. In fact, the axes of the entire body are under genetic regulation; a phenomenon called pattern formation 11 under the influ-ence of an organizer region of the body plan, including the teeth. Commonly, however, the body plan undergoes environmental perturba-RESULTS The patient reported that the DNA appliance was comfortable and there was no pain while wear-ing it. Arch development and bony remodeling of the palate necessitated periodic acrylic adjustments. After 7 weeks with one maxillary, acrylic-based DNA appliance, a significant improve-ment in lip posture/morphology and vertical maxillary excess was noted (Fig. 4). After 9 months of DNA appliance therapy and 8 months of fixed orthodontics, the patient was very pleased with the clinical results (Fig. 5), which included a wider smile, no ‘gummy smile’, anterior teeth able to couple for the first time (Fig. 6), and she reported no incidents of gagging, choking or coughing during sleep. 32 July/August 2013 JAOS tions, producing malocclusions. 12 The DNA appliance system puta-tively uses a biomimetic approach to address these issues, invoking the concept of epigenetic orthodontics or gene-environmental interactions. Anterior open bite can be divided into two etiologic cate-gories: skeletal and dento-alveolar. Thus, therapeutic success relies on both structural and functional reha-bilitation to guarantee stability of treatment. 13 Indeed, conventional treatment modalities for an AOB usually include orthodontic treat-ment combined with orthognathic surgery, but other restorative options for treatment can be successful. 14 However, alternative methods that harness physiologic processes might also be advanta-geous. For example, Chate and Falconer 15 used a simple orthodon-tic method to achieve re-intrusion of over-erupted teeth that were associated with AOB. More typi-cally, a combined orthodontic-orthognathic protocol is used to correct AOB. However, Jensen and Ruf 16 evaluated the short-term success of combined orthodontic-surgical correction of AOB. They concluded that normal overjet and overbite with proper incisal contact is achieved in only 40% of subjects using that approach. Yet another approach in the correction of AOB is the use of temporary anchorage devices (TADs). For example, Wald-man 17 used orthodontic TADs to provide a novel alternative to orthognathic surgery. The TADs provided skeletal anchorage for maxillary molar intrusion, allowing mandibular autorotation and subse-quent open-bite closure. However, orthodontic mechanics were still needed at every stage in that case, unlike the case that we report here. Another difference in the protocol that we adopt here is the integra-tion of an oral myofunctional ther-apist. Smithpeter and Covell 18 reported that OMT in conjunction with orthodontic treatment is highly effective in maintaining closure of AOB compared with orthodontic treatment alone. There-fore, we anticipate a stable result in this case; however, long-term review
Journal of the American Orthodontic Society July-August 2013 Buyer's Guide: Page 32