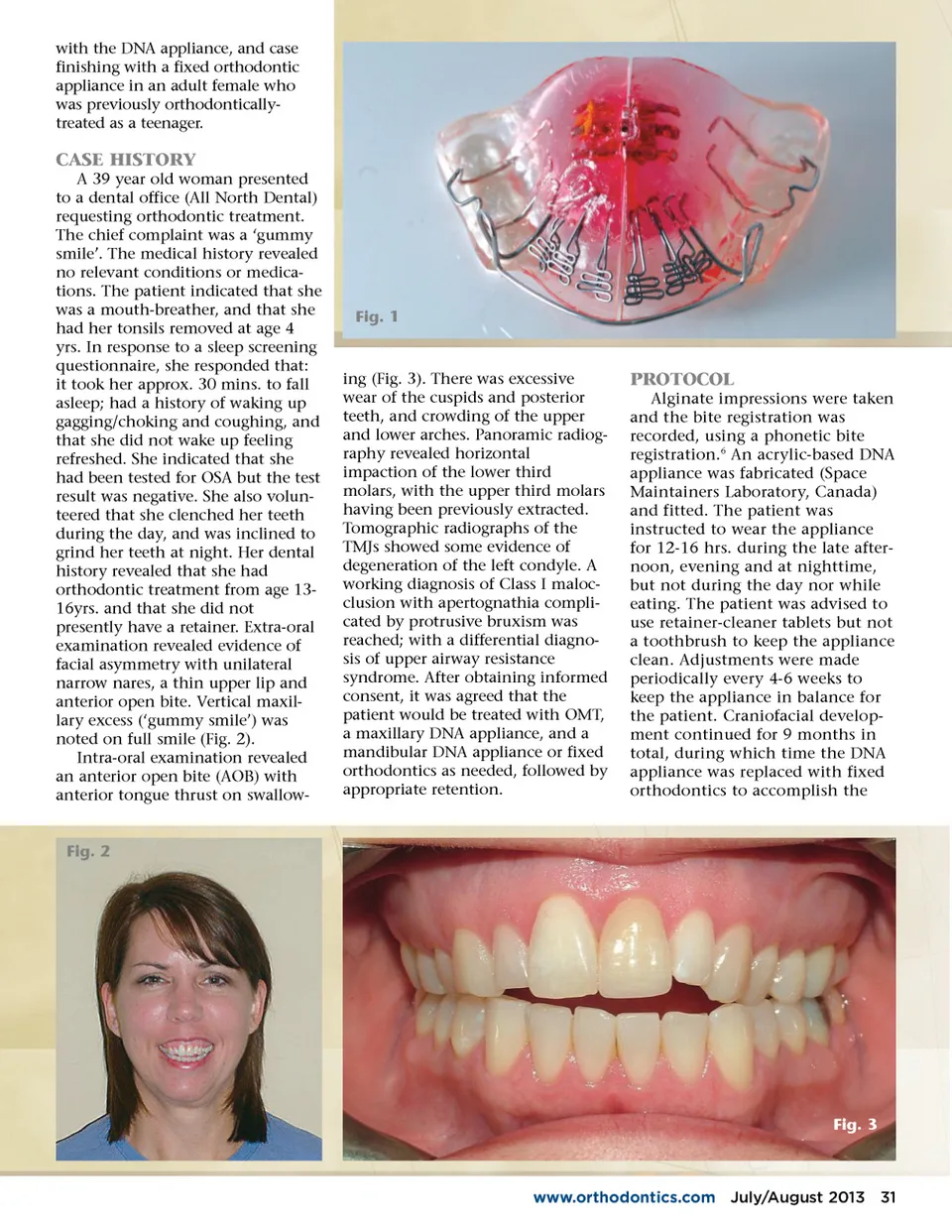
Using The DNA Appliance By G. Dave Singh, DDSc, PhD, BDS and William G. Harris, BSc, DDS ® T raditionally, orthodontists have used fixed appliances to apply forces to move teeth. The disadvantage of this approach is that inflammatory pathways are activated 1 , which induce discomfort throughout the treatment. Furthermore, the tacit assumption is that when the teeth are leveled, aligned and rotated, the patient will be in a better state of oral health. However, there are other co-morbid conditions associ-ated with malocclusions, such as temporo-mandibular joint (TMJ) dysfunction/headaches, snoring/obstructive sleep apnea 30 July/August 2013 JAOS (OSA) etc. that are often inadver-tently overlooked or ignored. There-fore, it might be better to take a more holistic approach and provide a more thorough craniofacial correction rather than attempt to treat the teeth in isolation. Indeed, while many cases are initially treated successfully, orthodontists know that relapse can occur after treatment. The reasons for relapse are complex and remain incom-pletely understood. Non-extraction protocols appeal to many clinicians practicing modern-day orthodontic correction as a way to reconcile dental and skeletal tissue relationships. In this regard, the DNA appliance system is designed to correct maxillo-mandibular underdevelopment in both children 2 and adults. 3-4 The acrylic-based DNA appliance (Fig. 1) typically has: 6 (patented) anterior 3-D axial springs TM , a midline screw, posterior occlusal coverage, retentive clasps, and a labial bow. The DNA appliance is preferentially worn for approx. 12-16 hrs. during the after-noon, evening and at nighttime, but not during the day and not while eating, partly in line with the circa-dian rhythm of tooth eruption. 5 The aim of this study is to report the effects of oral myofunctional therapy (OMT), craniofacial development
Journal of the American Orthodontic Society July-August 2013 Buyer's Guide: Page 30