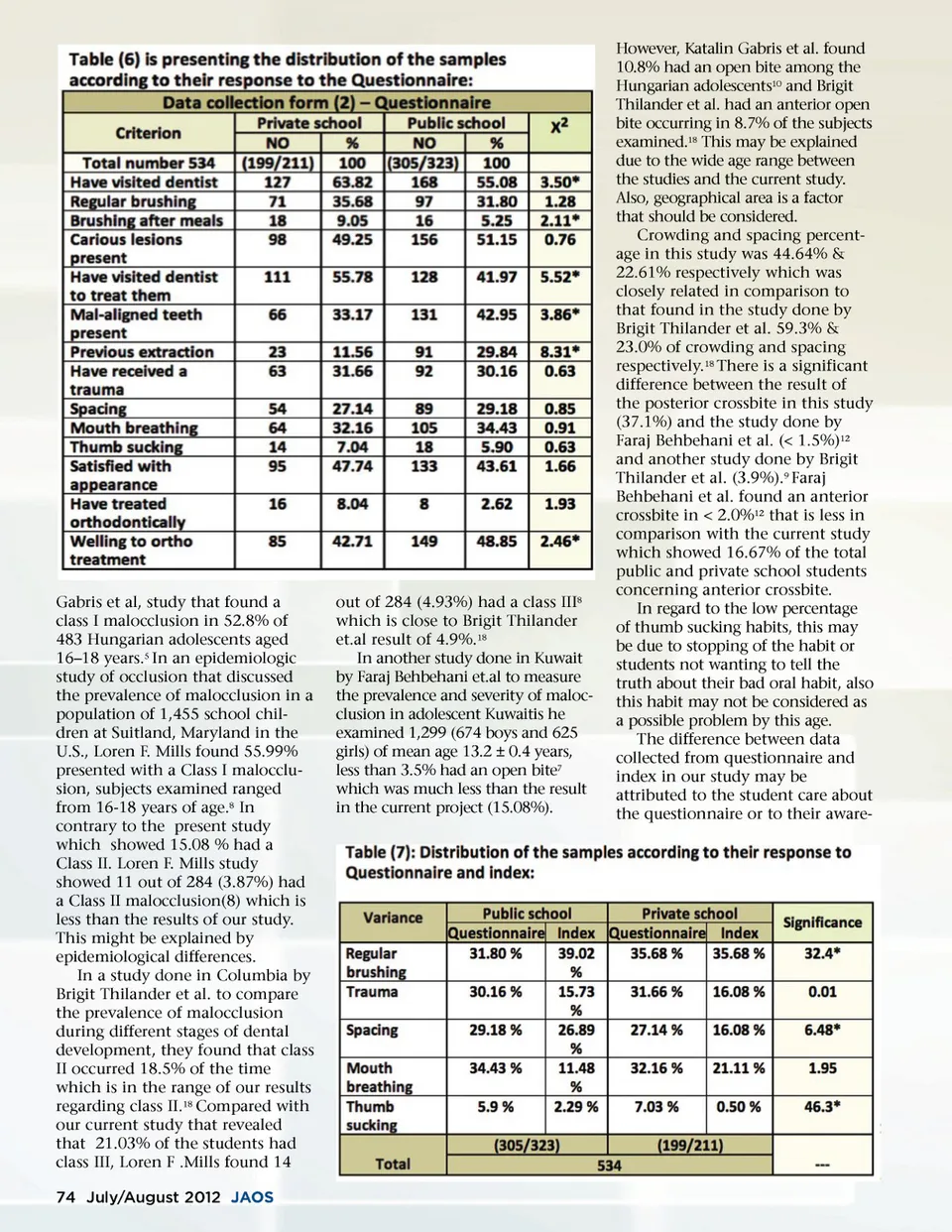
Gabris et al, study that found a class I malocclusion in 52.8% of 483 Hungarian adolescents aged 16–18 years. 5 In an epidemiologic study of occlusion that discussed the prevalence of malocclusion in a population of 1,455 school chil-dren at Suitland, Maryland in the U.S., Loren F. Mills found 55.99% presented with a Class I malocclu-sion, subjects examined ranged from 16-18 years of age. 8 In contrary to the present study which showed 15.08 % had a Class II. Loren F. Mills study showed 11 out of 284 (3.87%) had a Class II malocclusion(8) which is less than the results of our study. This might be explained by epidemiological differences. In a study done in Columbia by Brigit Thilander et al. to compare the prevalence of malocclusion during different stages of dental development, they found that class II occurred 18.5% of the time which is in the range of our results regarding class II. 18 Compared with our current study that revealed that 21.03% of the students had class III, Loren F .Mills found 14 74 July/August 2012 JAOS out of 284 (4.93%) had a class III 8 which is close to Brigit Thilander et.al result of 4.9%. 18 In another study done in Kuwait by Faraj Behbehani et.al to measure the prevalence and severity of maloc-clusion in adolescent Kuwaitis he examined 1,299 (674 boys and 625 girls) of mean age 13.2 ± 0.4 years, less than 3.5% had an open bite 7 which was much less than the result in the current project (15.08%). However, Katalin Gabris et al. found 10.8% had an open bite among the Hungarian adolescents 10 and Brigit Thilander et al. had an anterior open bite occurring in 8.7% of the subjects examined. 18 This may be explained due to the wide age range between the studies and the current study. Also, geographical area is a factor that should be considered. Crowding and spacing percent-age in this study was 44.64% & 22.61% respectively which was closely related in comparison to that found in the study done by Brigit Thilander et al. 59.3% & 23.0% of crowding and spacing respectively. 18 There is a significant difference between the result of the posterior crossbite in this study (37.1%) and the study done by Faraj Behbehani et al. (< 1.5%) 12 and another study done by Brigit Thilander et al. (3.9%). 9 Faraj Behbehani et al. found an anterior crossbite in < 2.0% 12 that is less in comparison with the current study which showed 16.67% of the total public and private school students concerning anterior crossbite. In regard to the low percentage of thumb sucking habits, this may be due to stopping of the habit or students not wanting to tell the truth about their bad oral habit, also this habit may not be considered as a possible problem by this age. The difference between data collected from questionnaire and index in our study may be attributed to the student care about the questionnaire or to their aware-
Journal of the American Orthodontic Society July-August 2012 Buyer's Guide: Page 74