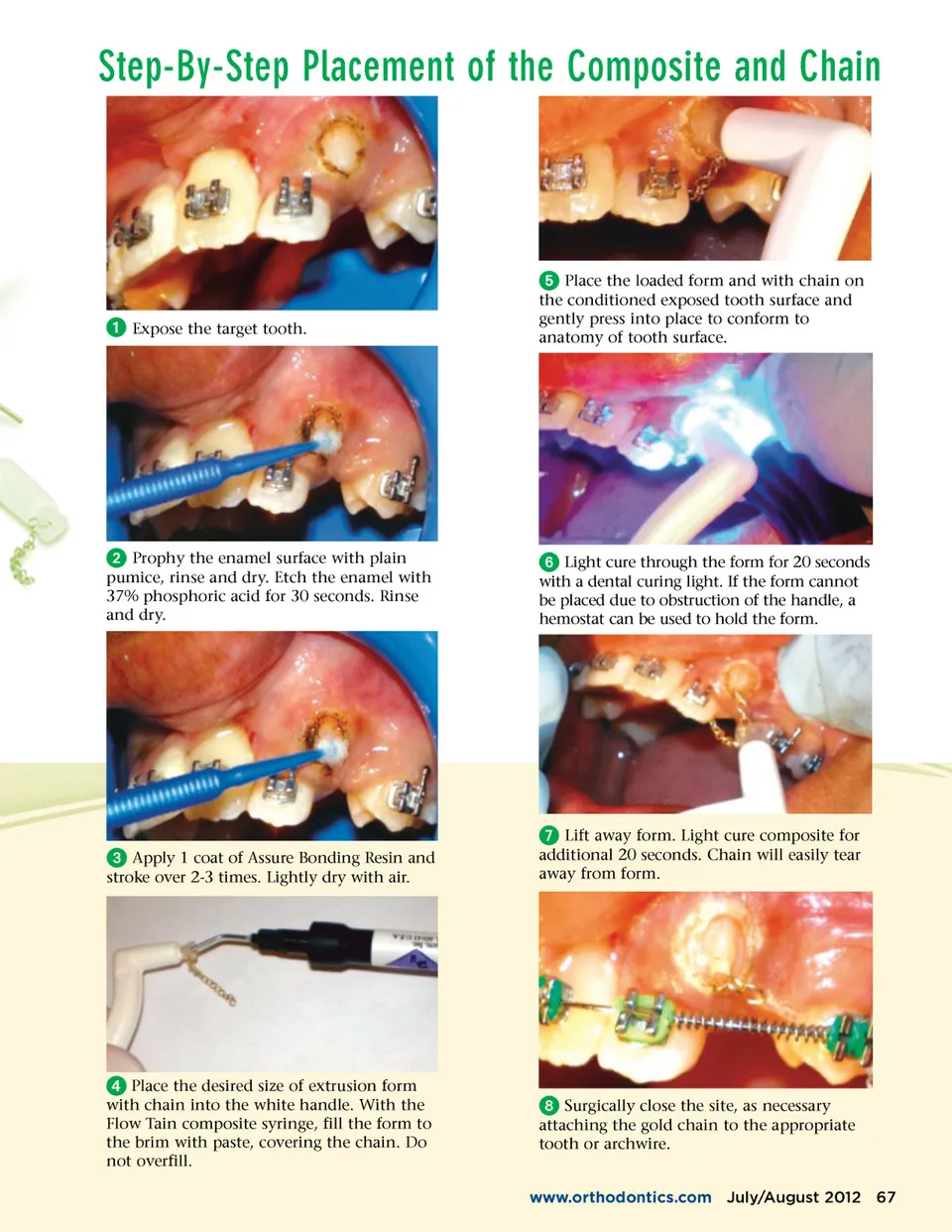
THE COMPOSITE-AND-CHAIN ™ ™ By Paul Gange he current technique for attaching a gold extru-sion chain to an impacted tooth for the purpose of extrusion involves bonding a mesh-based eyelet or bracket to the target tooth. Depending upon surgical acces-sibility, often the mesh base doesn’t fit flat against the exposed surface tooth anatomy, which can result in a weak bond and possible failure. This failure can require a repeat of the surgical procedure to re-bond the attachment to the tooth. Later, when the tooth has been extruded, the eyelet or bracket must be removed. The type of attachment is typically removed by pinching the base to fracture the composite bond to the metal mesh. This process can be very painful for the patient because these teeth have a tendency to be particu-larly sensitive. At times, the entire metal attachment needs to be ground away and this can be both time consuming for the dentist and uncomfortable for the patient. The metal-mesh base attach-ment approach can present diffi-culties for the oral surgeon or Extr u sion Kit T dentist. Once the tissue has been resected to expose the impacted tooth, the attachment is often bonded in a restricted and often-times moist environment. Since the clinician can’t contour the bracket pad to the anatomy of the tooth, its long-term retention can be compromised by the poor fit of metal-mesh base against the exposed tooth surface. The Composite-and-Chain TM Extrusion Kit, developed by Dr. James Hilgers, makes this proce-dure simpler for both the oral surgeon and the orthodontist. Its intention is to avoid the metal-mesh base altogether. Instead of utilizing a metal/mesh bonding pad to secure the chain, the C&C kit uses a pod of polymer-ized composite formed to the exact available anatomy of the tooth and in which the 14k gold chain is integrally embedded. There are 2 configurations of clear silicone molds which form oval (small) or rectangular (large) composite pods, depending on the surface area available to the surgeon. The translucent silicone mold allows direct exposure to a curing light and permits complete curing of the compos-ite pod. The malleable walls of the silicone form allow the composite to contour easily to the exposed anatomy of the target tooth. The composite cures to a smooth glassine surface so that there are no residual rough edges to compro-mise tissue healing. The enamel primer included in the kit (Assure Universal Bonding Resin) is hydrophilic so slight moisture on the etched enamel surface will still result in a secure bond. Because the chain is completely encapsulated in the polymerized composite, extrusion forces can be applied with less concern for bond failure. Most importantly, once the tooth has been moved into its proper place in the dental arch, removal of the composite pod is easy for both the orthodontist and the patient. The composite pod and encap-sulated chain is simply smoothed off the tooth surface with a diamond bur. This avoids the painful crimping or fracturing of the attachment, which can be the source of severe patient discomfort. The next page presents an illustrated example for placement of the Composite-and-Chain TM . 66 July/August 2012 JAOS
Journal of the American Orthodontic Society July-August 2012 Buyer's Guide: Page 66