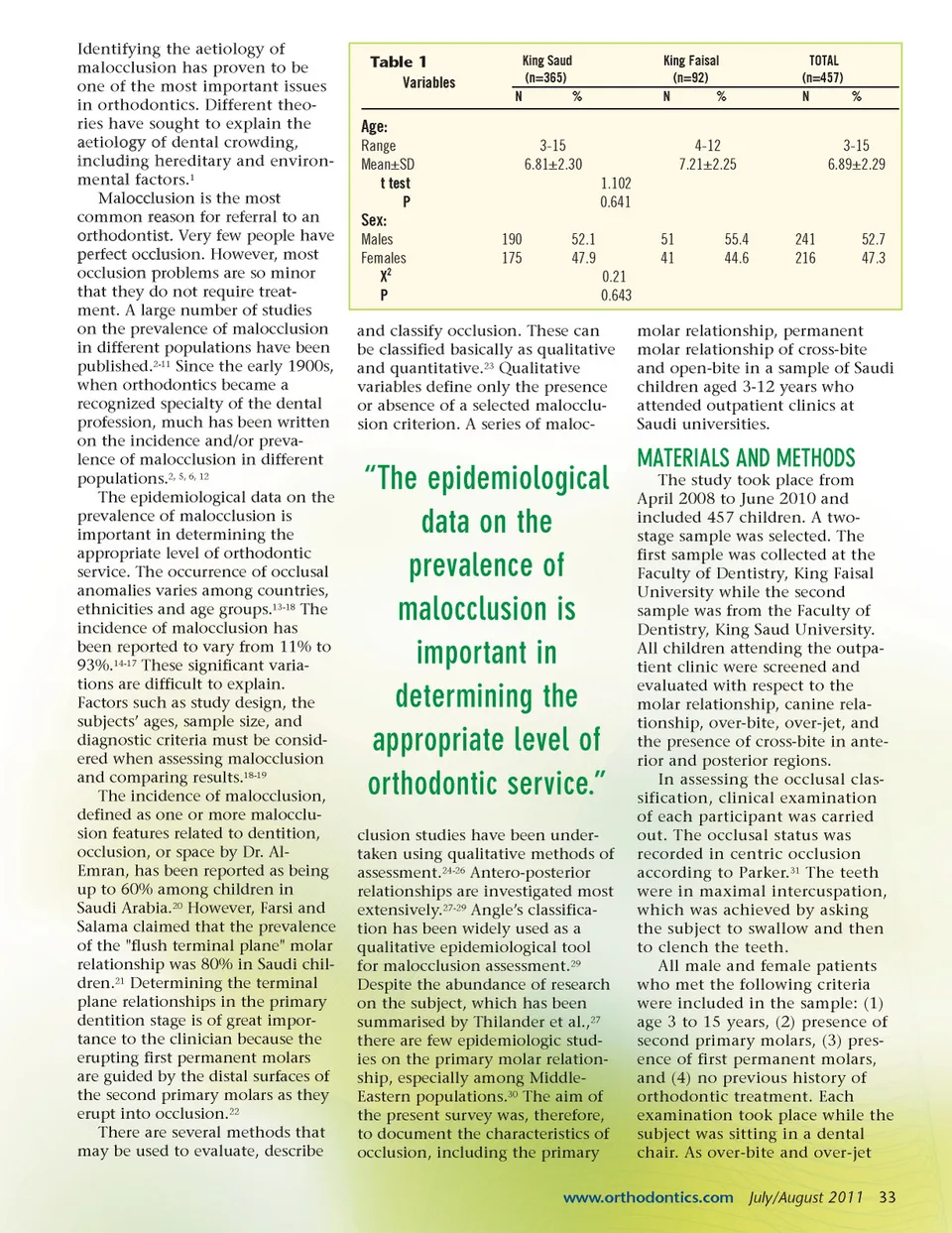
Identifying the aetiology of malocclusion has proven to be one of the most important issues in orthodontics. Different theo-ries have sought to explain the aetiology of dental crowding, including hereditary and environ-mental factors. 1 Malocclusion is the most common reason for referral to an orthodontist. Very few people have perfect occlusion. However, most occlusion problems are so minor that they do not require treat-ment. A large number of studies on the prevalence of malocclusion in different populations have been published. 2-11 Since the early 1900s, when orthodontics became a recognized specialty of the dental profession, much has been written on the incidence and/or preva-lence of malocclusion in different populations. 2, 5, 6, 12 The epidemiological data on the prevalence of malocclusion is important in determining the appropriate level of orthodontic service. The occurrence of occlusal anomalies varies among countries, ethnicities and age groups. 13-18 The incidence of malocclusion has been reported to vary from 11% to 93%. 14-17 These significant varia-tions are difficult to explain. Factors such as study design, the subjects’ ages, sample size, and diagnostic criteria must be consid-ered when assessing malocclusion and comparing results. 18-19 The incidence of malocclusion, defined as one or more malocclu-sion features related to dentition, occlusion, or space by Dr. Al-Emran, has been reported as being up to 60% among children in Saudi Arabia. 20 However, Farsi and Salama claimed that the prevalence of the "flush terminal plane" molar relationship was 80% in Saudi chil-dren. 21 Determining the terminal plane relationships in the primary dentition stage is of great impor-tance to the clinician because the erupting first permanent molars are guided by the distal surfaces of the second primary molars as they erupt into occlusion. 22 There are several methods that may be used to evaluate, describe Table 1 Variables King Saud (n=365) N% King Faisal (n=92) N % TOTAL (n=457) N % Age: Range Mean±SD t test P 3-15 6.81±2.30 1.102 0.641 190 175 52.1 47.9 0.21 0.643 molar relationship, permanent molar relationship of cross-bite and open-bite in a sample of Saudi children aged 3-12 years who attended outpatient clinics at Saudi universities. 51 41 55.4 44.6 241 216 52.7 47.3 4-12 7.21±2.25 3-15 6.89±2.29 Sex: Males Females X 2 P and classify occlusion. These can be classified basically as qualitative and quantitative. 23 Qualitative variables define only the presence or absence of a selected malocclu-sion criterion. A series of maloc-“The epidemiological data on the prevalence of malocclusion is important in determining the appropriate level of orthodontic service.” clusion studies have been under-taken using qualitative methods of assessment. 24-26 Antero-posterior relationships are investigated most extensively. 27-29 Angle’s classifica-tion has been widely used as a qualitative epidemiological tool for malocclusion assessment. 29 Despite the abundance of research on the subject, which has been summarised by Thilander et al., 27 there are few epidemiologic stud-ies on the primary molar relation-ship, especially among Middle-Eastern populations. 30 The aim of the present survey was, therefore, to document the characteristics of occlusion, including the primary MATERIALS AND METHODS The study took place from April 2008 to June 2010 and included 457 children. A two-stage sample was selected. The first sample was collected at the Faculty of Dentistry, King Faisal University while the second sample was from the Faculty of Dentistry, King Saud University. All children attending the outpa-tient clinic were screened and evaluated with respect to the molar relationship, canine rela-tionship, over-bite, over-jet, and the presence of cross-bite in ante-rior and posterior regions. In assessing the occlusal clas-sification, clinical examination of each participant was carried out. The occlusal status was recorded in centric occlusion according to Parker. 31 The teeth were in maximal intercuspation, which was achieved by asking the subject to swallow and then to clench the teeth. All male and female patients who met the following criteria were included in the sample: (1) age 3 to 15 years, (2) presence of second primary molars, (3) pres-ence of first permanent molars, and (4) no previous history of orthodontic treatment. Each examination took place while the subject was sitting in a dental chair. As over-bite and over-jet www.orthodontics.com July/August 2011 33
Journal of the American Orthodontic Society July-August 2011-Buyer's Guide: Page 33