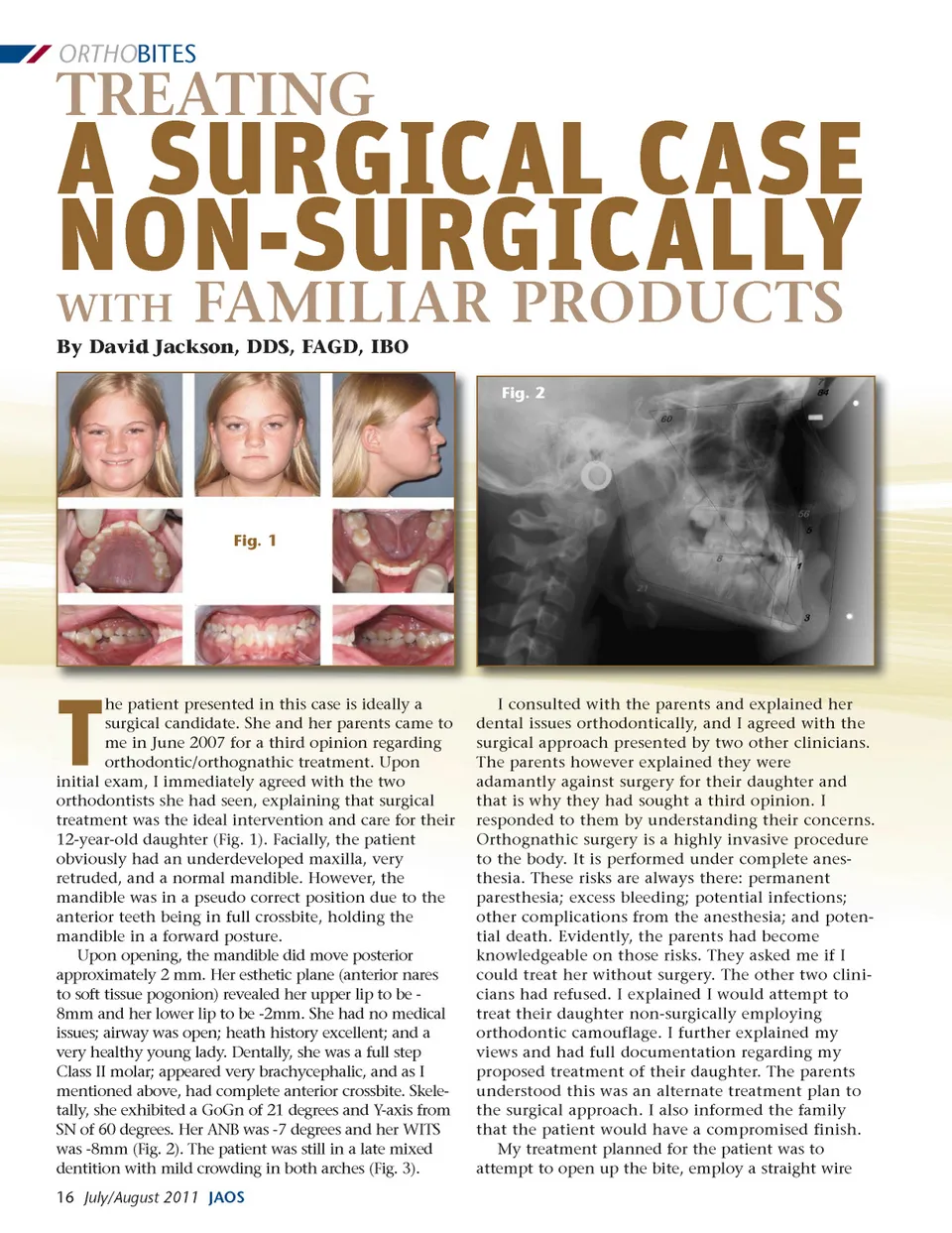
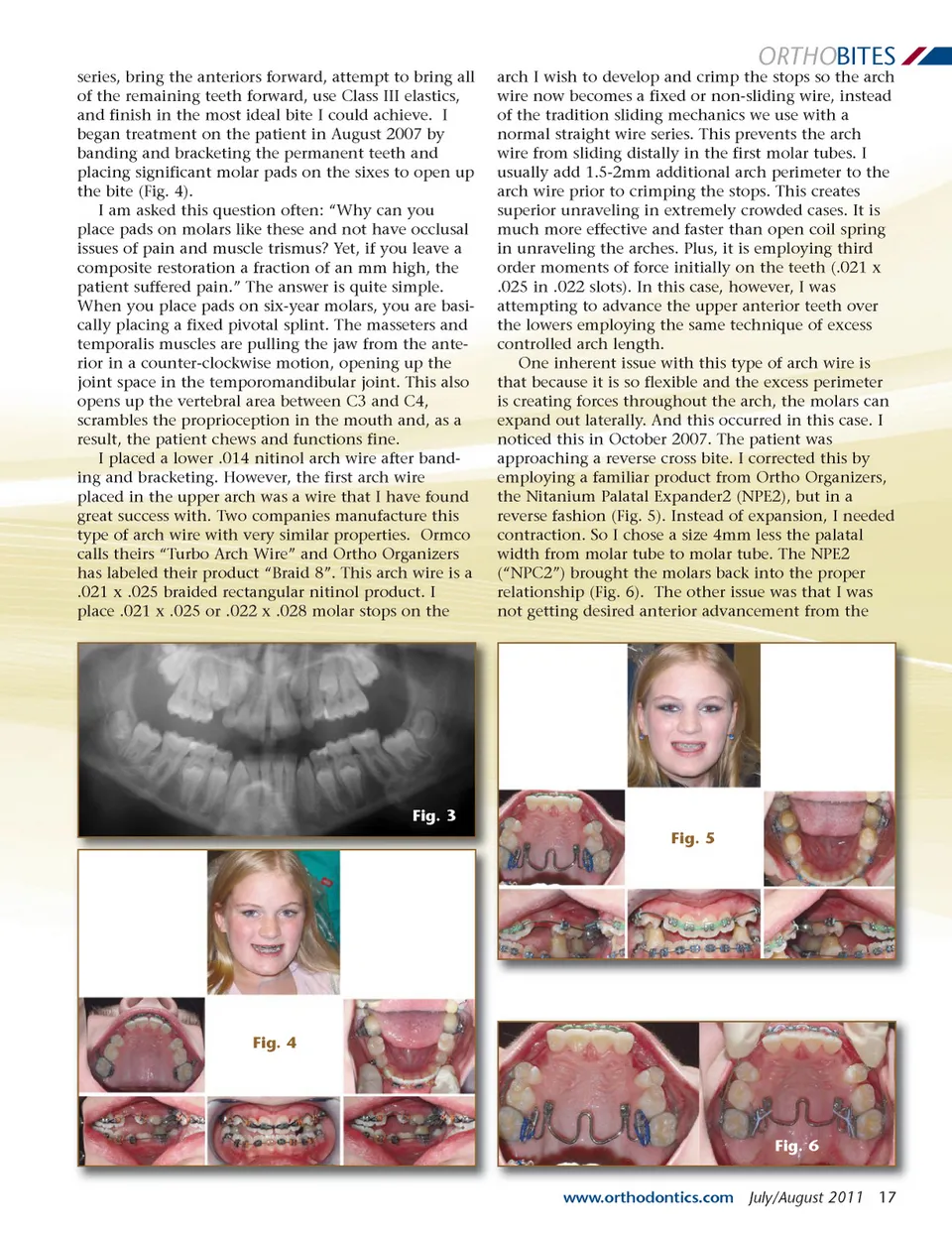
ORTHO BITES A SURGICAL CASE NON-SURGICALLY WITH TREATING FAMILIAR PRODUCTS Fig. 2 By David Jackson, DDS, FAGD, IBO Fig. 1 he patient presented in this case is ideally a surgical candidate. She and her parents came to me in June 2007 for a third opinion regarding orthodontic/orthognathic treatment. Upon initial exam, I immediately agreed with the two orthodontists she had seen, explaining that surgical treatment was the ideal intervention and care for their 12-year-old daughter (Fig. 1). Facially, the patient obviously had an underdeveloped maxilla, very retruded, and a normal mandible. However, the mandible was in a pseudo correct position due to the anterior teeth being in full crossbite, holding the mandible in a forward posture. Upon opening, the mandible did move posterior approximately 2 mm. Her esthetic plane (anterior nares to soft tissue pogonion) revealed her upper lip to be -8mm and her lower lip to be -2mm. She had no medical issues; airway was open; heath history excellent; and a very healthy young lady. Dentally, she was a full step Class II molar; appeared very brachycephalic, and as I mentioned above, had complete anterior crossbite. Skele-tally, she exhibited a GoGn of 21 degrees and Y-axis from SN of 60 degrees. Her ANB was -7 degrees and her WITS was -8mm (Fig. 2). The patient was still in a late mixed dentition with mild crowding in both arches (Fig. 3). T I consulted with the parents and explained her dental issues orthodontically, and I agreed with the surgical approach presented by two other clinicians. The parents however explained they were adamantly against surgery for their daughter and that is why they had sought a third opinion. I responded to them by understanding their concerns. Orthognathic surgery is a highly invasive procedure to the body. It is performed under complete anes-thesia. These risks are always there: permanent paresthesia; excess bleeding; potential infections; other complications from the anesthesia; and poten-tial death. Evidently, the parents had become knowledgeable on those risks. They asked me if I could treat her without surgery. The other two clini-cians had refused. I explained I would attempt to treat their daughter non-surgically employing orthodontic camouflage. I further explained my views and had full documentation regarding my proposed treatment of their daughter. The parents understood this was an alternate treatment plan to the surgical approach. I also informed the family that the patient would have a compromised finish. My treatment planned for the patient was to attempt to open up the bite, employ a straight wire 16 July/August 2011 JAOS
Journal of the American Orthodontic Society July-August 2011-Buyer's Guide: Page 16