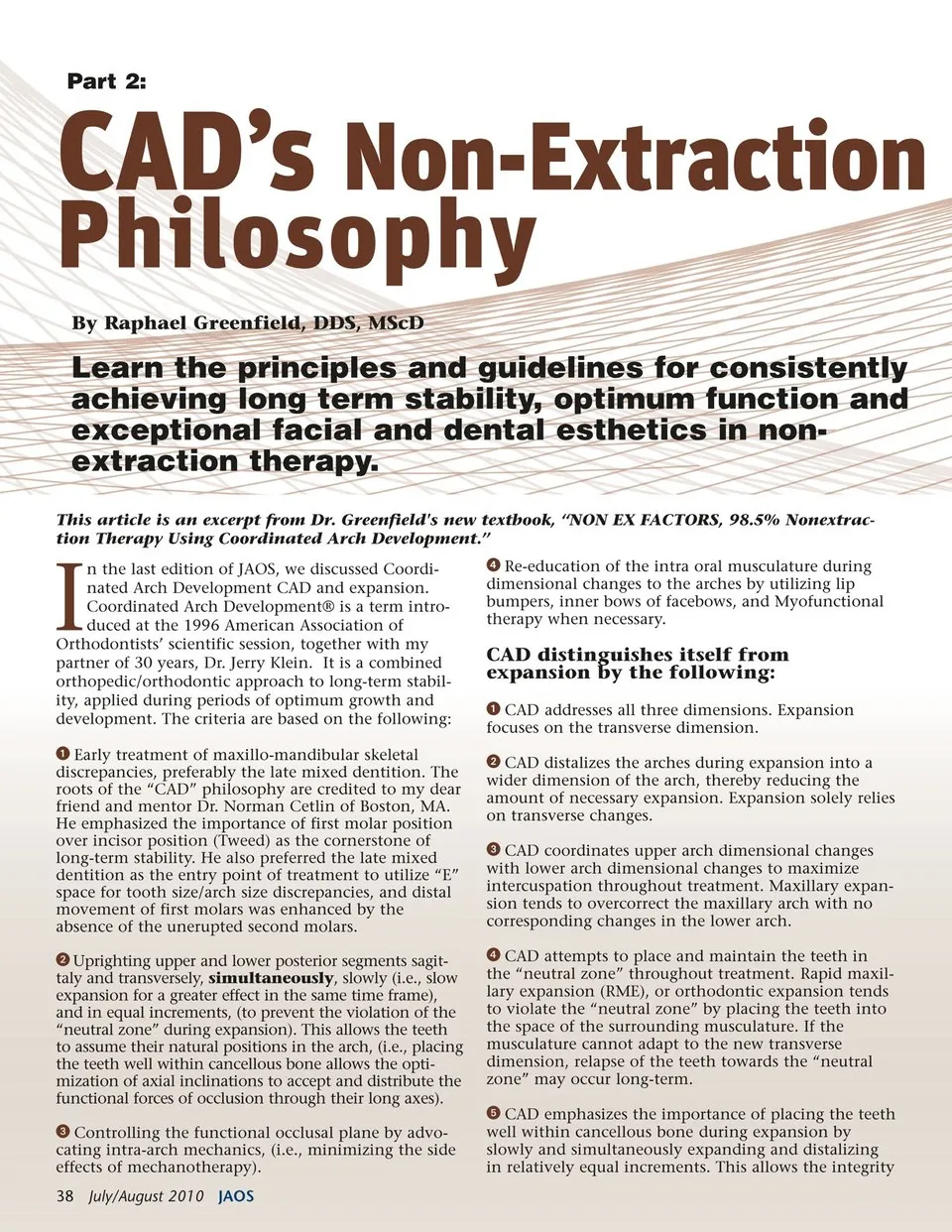
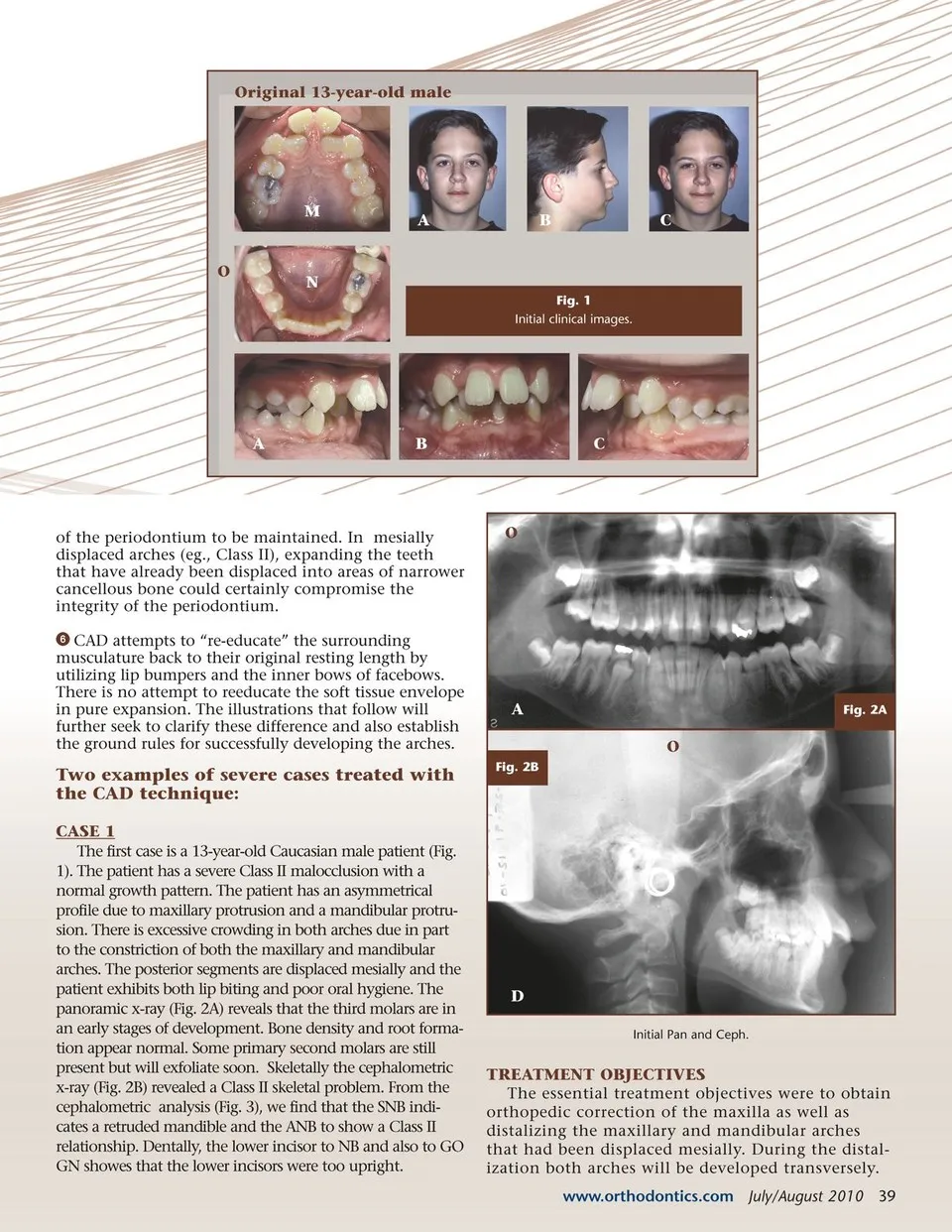
Part 2: CAD’s Non-Extraction Philosophy By Raphael Greenfield, DDS, MScD Learn the principles and guidelines for consistently achieving long term stability, optimum function and exceptional facial and dental esthetics in non-extraction therapy. This article is an excerpt from Dr. Greenfield's new textbook, “NON EX FACTORS, 98.5% Nonextrac-tion Therapy Using Coordinated Arch Development.” I n the last edition of JAOS, we discussed Coordi-nated Arch Development CAD and expansion. Coordinated Arch Development® is a term intro-duced at the 1996 American Association of Orthodontists’ scientific session, together with my partner of 30 years, Dr. Jerry Klein. It is a combined orthopedic/orthodontic approach to long-term stabil-ity, applied during periods of optimum growth and development. The criteria are based on the following: Early treatment of maxillo-mandibular skeletal discrepancies, preferably the late mixed dentition. The roots of the “CAD” philosophy are credited to my dear friend and mentor Dr. Norman Cetlin of Boston, MA. He emphasized the importance of first molar position over incisor position (Tweed) as the cornerstone of long-term stability. He also preferred the late mixed dentition as the entry point of treatment to utilize “E” space for tooth size/arch size discrepancies, and distal movement of first molars was enhanced by the absence of the unerupted second molars. Uprighting upper and lower posterior segments sagit-taly and transversely, simultaneously, slowly (i.e., slow expansion for a greater effect in the same time frame), and in equal increments, (to prevent the violation of the “neutral zone” during expansion). This allows the teeth to assume their natural positions in the arch, (i.e., placing the teeth well within cancellous bone allows the opti-mization of axial inclinations to accept and distribute the functional forces of occlusion through their long axes). Controlling the functional occlusal plane by advo-cating intra-arch mechanics, (i.e., minimizing the side effects of mechanotherapy). 38 July/August 2010 JAOS Re-education of the intra oral musculature during dimensional changes to the arches by utilizing lip bumpers, inner bows of facebows, and Myofunctional therapy when necessary. CAD distinguishes itself from expansion by the following: CAD addresses all three dimensions. Expansion focuses on the transverse dimension. CAD distalizes the arches during expansion into a wider dimension of the arch, thereby reducing the amount of necessary expansion. Expansion solely relies on transverse changes. CAD coordinates upper arch dimensional changes with lower arch dimensional changes to maximize intercuspation throughout treatment. Maxillary expan-sion tends to overcorrect the maxillary arch with no corresponding changes in the lower arch. CAD attempts to place and maintain the teeth in the “neutral zone” throughout treatment. Rapid maxil-lary expansion (RME), or orthodontic expansion tends to violate the “neutral zone” by placing the teeth into the space of the surrounding musculature. If the musculature cannot adapt to the new transverse dimension, relapse of the teeth towards the “neutral zone” may occur long-term. CAD emphasizes the importance of placing the teeth well within cancellous bone during expansion by slowly and simultaneously expanding and distalizing in relatively equal increments. This allows the integrity
Journal of the American Orthodontic Society July-August 2010/Buyer's Guide: Page 38