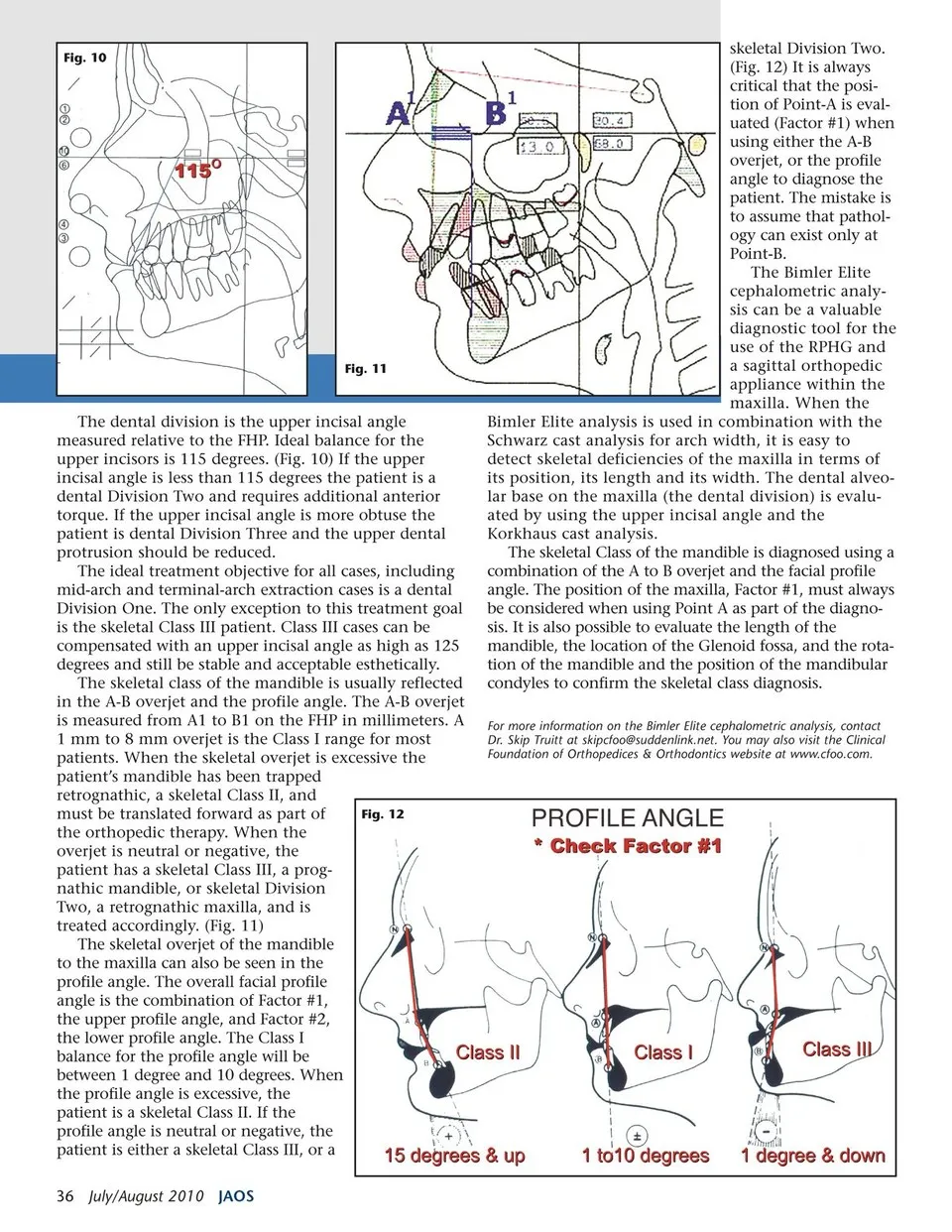
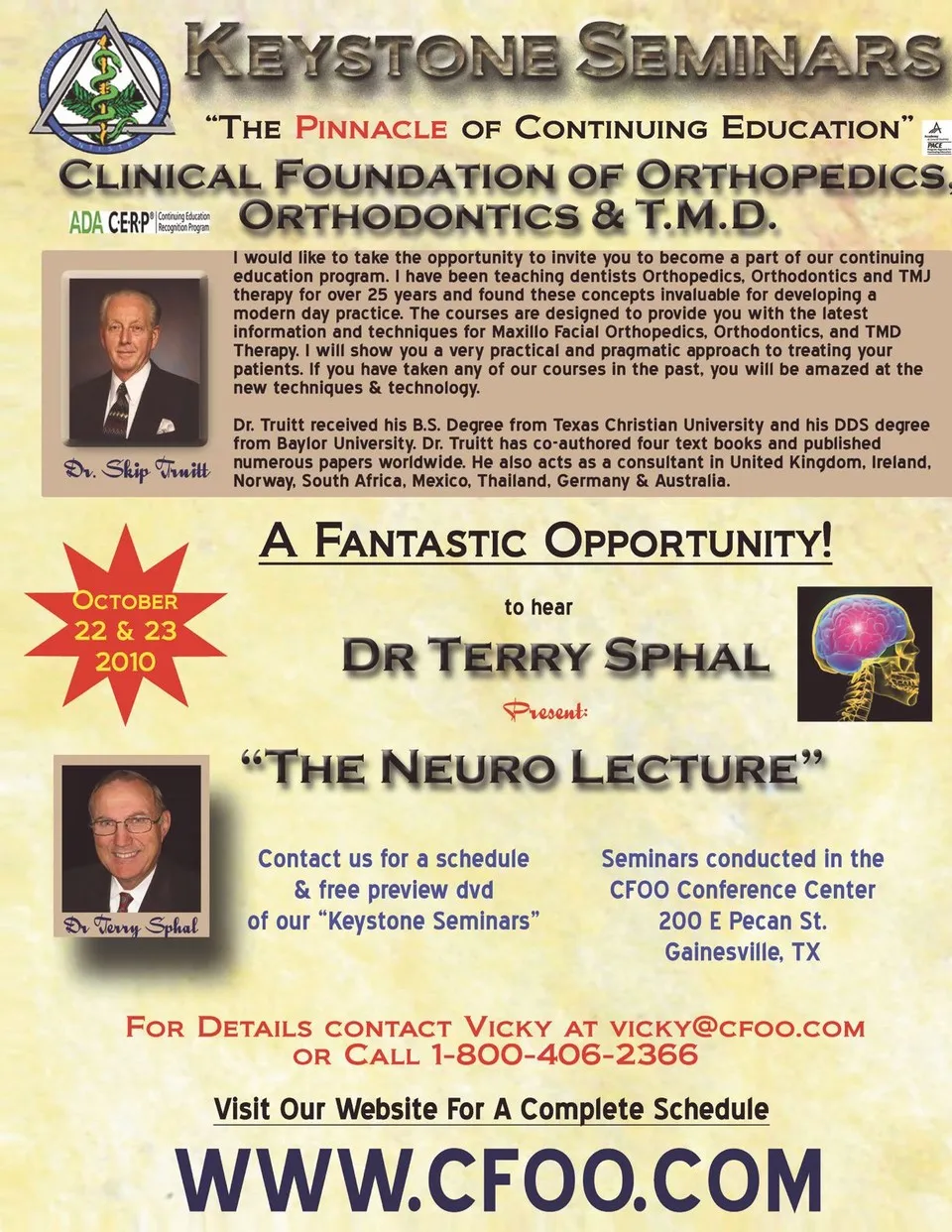
Fig. 10 skeletal Division Two. (Fig. 12) It is always critical that the posi-tion of Point-A is eval-uated (Factor #1) when using either the A-B overjet, or the profile angle to diagnose the patient. The mistake is to assume that pathol-ogy can exist only at Point-B. Fig. 11 The dental division is the upper incisal angle measured relative to the FHP. Ideal balance for the upper incisors is 115 degrees. (Fig. 10) If the upper incisal angle is less than 115 degrees the patient is a dental Division Two and requires additional anterior torque. If the upper incisal angle is more obtuse the patient is dental Division Three and the upper dental protrusion should be reduced. The ideal treatment objective for all cases, including mid-arch and terminal-arch extraction cases is a dental Division One. The only exception to this treatment goal is the skeletal Class III patient. Class III cases can be compensated with an upper incisal angle as high as 125 degrees and still be stable and acceptable esthetically. The skeletal class of the mandible is usually reflected in the A-B overjet and the profile angle. The A-B overjet is measured from A1 to B1 on the FHP in millimeters. A 1 mm to 8 mm overjet is the Class I range for most patients. When the skeletal overjet is excessive the patient’s mandible has been trapped retrognathic, a skeletal Class II, and must be translated forward as part of the orthopedic therapy. When the overjet is neutral or negative, the patient has a skeletal Class III, a prog-nathic mandible, or skeletal Division Two, a retrognathic maxilla, and is treated accordingly. (Fig. 11) The skeletal overjet of the mandible to the maxilla can also be seen in the profile angle. The overall facial profile angle is the combination of Factor #1, the upper profile angle, and Factor #2, the lower profile angle. The Class I balance for the profile angle will be between 1 degree and 10 degrees. When the profile angle is excessive, the patient is a skeletal Class II. If the profile angle is neutral or negative, the patient is either a skeletal Class III, or a Fig. 12 36 July/August 2010 JAOS The Bimler Elite cephalometric analy-sis can be a valuable diagnostic tool for the use of the RPHG and a sagittal orthopedic appliance within the maxilla. When the Bimler Elite analysis is used in combination with the Schwarz cast analysis for arch width, it is easy to detect skeletal deficiencies of the maxilla in terms of its position, its length and its width. The dental alveo-lar base on the maxilla (the dental division) is evalu-ated by using the upper incisal angle and the Korkhaus cast analysis. The skeletal Class of the mandible is diagnosed using a combination of the A to B overjet and the facial profile angle. The position of the maxilla, Factor #1, must always be considered when using Point A as part of the diagno-sis. It is also possible to evaluate the length of the mandible, the location of the Glenoid fossa, and the rota-tion of the mandible and the position of the mandibular condyles to confirm the skeletal class diagnosis. For more information on the Bimler Elite cephalometric analysis, contact Dr. Skip Truitt at skipcfoo@suddenlink.net. You may also visit the Clinical Foundation of Orthopedices & Orthodontics website at www.cfoo.com.
Journal of the American Orthodontic Society July-August 2010/Buyer's Guide: Page 36