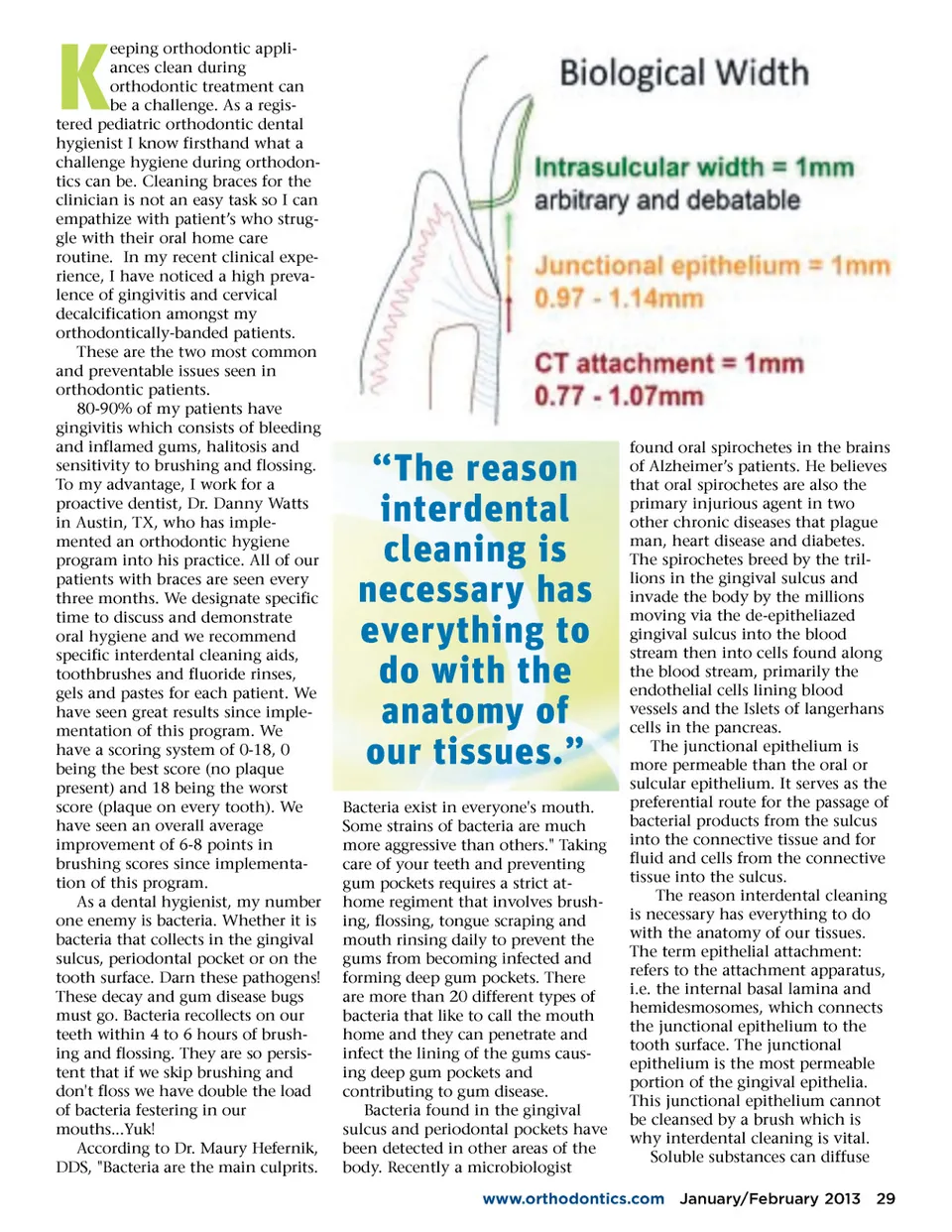
eeping orthodontic appli-ances clean during orthodontic treatment can be a challenge. As a regis-tered pediatric orthodontic dental hygienist I know firsthand what a challenge hygiene during orthodon-tics can be. Cleaning braces for the clinician is not an easy task so I can empathize with patient’s who strug-gle with their oral home care routine. In my recent clinical expe-rience, I have noticed a high preva-lence of gingivitis and cervical decalcification amongst my orthodontically-banded patients. These are the two most common and preventable issues seen in orthodontic patients. 80-90% of my patients have gingivitis which consists of bleeding and inflamed gums, halitosis and sensitivity to brushing and flossing. To my advantage, I work for a proactive dentist, Dr. Danny Watts in Austin, TX, who has imple-mented an orthodontic hygiene program into his practice. All of our patients with braces are seen every three months. We designate specific time to discuss and demonstrate oral hygiene and we recommend specific interdental cleaning aids, toothbrushes and fluoride rinses, gels and pastes for each patient. We have seen great results since imple-mentation of this program. We have a scoring system of 0-18, 0 being the best score (no plaque present) and 18 being the worst score (plaque on every tooth). We have seen an overall average improvement of 6-8 points in brushing scores since implementa-tion of this program. As a dental hygienist, my number one enemy is bacteria. Whether it is bacteria that collects in the gingival sulcus, periodontal pocket or on the tooth surface. Darn these pathogens! These decay and gum disease bugs must go. Bacteria recollects on our teeth within 4 to 6 hours of brush-ing and flossing. They are so persis-tent that if we skip brushing and don't floss we have double the load of bacteria festering in our mouths...Yuk! According to Dr. Maury Hefernik, DDS, "Bacteria are the main culprits. K “The reason interdental cleaning is necessary has everything to do with the anatomy of our tissues.” Bacteria exist in everyone's mouth. Some strains of bacteria are much more aggressive than others." Taking care of your teeth and preventing gum pockets requires a strict at-home regiment that involves brush-ing, flossing, tongue scraping and mouth rinsing daily to prevent the gums from becoming infected and forming deep gum pockets. There are more than 20 different types of bacteria that like to call the mouth home and they can penetrate and infect the lining of the gums caus-ing deep gum pockets and contributing to gum disease. Bacteria found in the gingival sulcus and periodontal pockets have been detected in other areas of the body. Recently a microbiologist found oral spirochetes in the brains of Alzheimer’s patients. He believes that oral spirochetes are also the primary injurious agent in two other chronic diseases that plague man, heart disease and diabetes. The spirochetes breed by the tril-lions in the gingival sulcus and invade the body by the millions moving via the de-epitheliazed gingival sulcus into the blood stream then into cells found along the blood stream, primarily the endothelial cells lining blood vessels and the Islets of langerhans cells in the pancreas. The junctional epithelium is more permeable than the oral or sulcular epithelium. It serves as the preferential route for the passage of bacterial products from the sulcus into the connective tissue and for fluid and cells from the connective tissue into the sulcus. The reason interdental cleaning is necessary has everything to do with the anatomy of our tissues. The term epithelial attachment: refers to the attachment apparatus, i.e. the internal basal lamina and hemidesmosomes, which connects the junctional epithelium to the tooth surface. The junctional epithelium is the most permeable portion of the gingival epithelia. This junctional epithelium cannot be cleansed by a brush which is why interdental cleaning is vital. Soluble substances can diffuse www.orthodontics.com January/February 2013 29
Journal of the American Orthodontic Society January-February 2013: Page 29