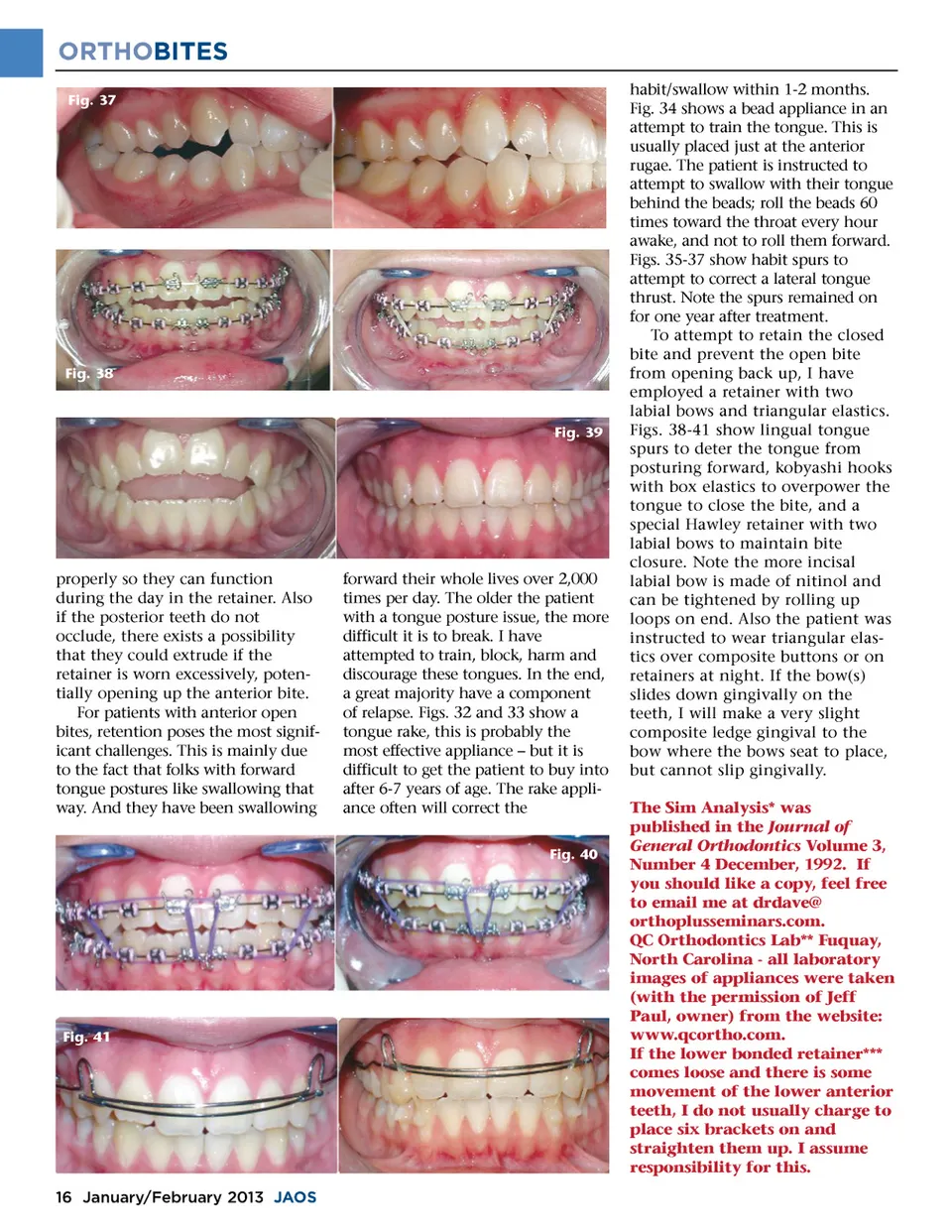
ORTHOBITES Fig. 37 Fig. 38 Fig. 39 properly so they can function during the day in the retainer. Also if the posterior teeth do not occlude, there exists a possibility that they could extrude if the retainer is worn excessively, poten-tially opening up the anterior bite. For patients with anterior open bites, retention poses the most signif-icant challenges. This is mainly due to the fact that folks with forward tongue postures like swallowing that way. And they have been swallowing forward their whole lives over 2,000 times per day. The older the patient with a tongue posture issue, the more difficult it is to break. I have attempted to train, block, harm and discourage these tongues. In the end, a great majority have a component of relapse. Figs. 32 and 33 show a tongue rake, this is probably the most effective appliance – but it is difficult to get the patient to buy into after 6-7 years of age. The rake appli-ance often will correct the Fig. 40 habit/swallow within 1-2 months. Fig. 34 shows a bead appliance in an attempt to train the tongue. This is usually placed just at the anterior rugae. The patient is instructed to attempt to swallow with their tongue behind the beads; roll the beads 60 times toward the throat every hour awake, and not to roll them forward. Figs. 35-37 show habit spurs to attempt to correct a lateral tongue thrust. Note the spurs remained on for one year after treatment. To attempt to retain the closed bite and prevent the open bite from opening back up, I have employed a retainer with two labial bows and triangular elastics. Figs. 38-41 show lingual tongue spurs to deter the tongue from posturing forward, kobyashi hooks with box elastics to overpower the tongue to close the bite, and a special Hawley retainer with two labial bows to maintain bite closure. Note the more incisal labial bow is made of nitinol and can be tightened by rolling up loops on end. Also the patient was instructed to wear triangular elas-tics over composite buttons or on retainers at night. If the bow(s) slides down gingivally on the teeth, I will make a very slight composite ledge gingival to the bow where the bows seat to place, but cannot slip gingivally. The Sim Analysis* was published in the Journal of General Orthodontics Volume 3, Number 4 December, 1992. If you should like a copy, feel free to email me at drdave@ orthoplusseminars.com. QC Orthodontics Lab** Fuquay, North Carolina -all laboratory images of appliances were taken (with the permission of Jeff Paul, owner) from the website: www.qcortho.com. If the lower bonded retainer*** comes loose and there is some movement of the lower anterior teeth, I do not usually charge to place six brackets on and straighten them up. I assume responsibility for this. Fig. 41 16 January/February 2013 JAOS
Journal of the American Orthodontic Society January-February 2013: Page 16